
Abstract
Purpose
Abiraterone acetate is used at a fixed oral dose of 1000 mg once daily (OD) taken fasted. By administering abiraterone acetate with food, a reduced dose can potentially be given while maintaining equivalent abiraterone exposure. Moreover, administering abiraterone acetate with a breakfast is considered more patient friendly. The aim of this study was to establish the bio-equivalent lower dose of abiraterone when taken with a continental breakfast (CB) compared to the standard intake of 1000 mg OD fasted.
Methods
In this phase I, randomized cross-over, multi-center study, abiraterone pharmacokinetics (PK) were evaluated in patients with metastatic castration-resistant prostate cancer who were treated for 14 days with 1000 mg abiraterone acetate taken fasted, followed by 14 days of treatment with 500 mg taken with a CB.
Results
14 patients were enrolled into the study, of whom 12 were eligible for PK analysis. The geometric mean ratio (GMR) (fed/fasted) was 0.88 (90% CI 0.73–1.07) for area-under-the-curve (AUC0–24h), 1.03 (90% CI 0.79–1.34) for Cmax and 0.81 (90% CI 0.60–1.10) for Ctrough, respectively. High inter-patient variability (> 50%) was found for all PK parameters under both intake conditions. Patients seemed to be slightly more satisfied about the intake of 500 mg abiraterone acetate when taken with a CB compared to 1000 mg fasted.
Conclusion
In conclusion, a bioequivalent lower dose of abiraterone taken with food could not be established in our study. Although based on the absence of a exposure–toxicity relationship, the strict bioequivalence margins as defined by the FDA guidelines could be applied more flexible for abiraterone. Information on the effect of food on abiraterone pharmacokinetics as presented in our study can be used for patients with difficulties taken their medication fasted.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
With the introduction of oral targeted anti-cancer drugs, the intake of food as a cause of intra-patient variability in drug absorption has become relevant. As part of the registration process of these new drugs, studies to quantify the effect of food on pharmacokinetics are routinely performed. When food affects drug absorption, the advised intake regime is often fasted for oncologists [1].
One of the drugs with an outspoken food effect is abiraterone acetate (AA) (Zytiga®). AA is a pro-drug of abiraterone. Abiraterone is a selective inhibitor of cytochrome (CYP) 17A1, a crucial enzyme in androgen biosynthesis, resulting in virtually undetectable serum and intra-tumor androgen levels and thereby resulting in antitumor activity in patients with locally advanced or metastatic prostate cancer (mHSPC and mCRPC) [2,3,4]. AA tablets are administered at a fixed oral dose of 1000 mg OD in a fasted state in combination with 10 mg prednis(ol)one daily [5].
Abiraterone acetate was developed to overcome the poor bioavailability of the initially formulated abiraterone. Nevertheless, also AA shows very limited bioavailability mainly due to its physiochemical properties of low solubility in aqueous media and low permeability properties [6]. The bioavailability of AA is majorly affected by ingestion with food. However, large differences in the influence of food on pharmacokinetics of AA are seen between different studies. Chi et al. showed that the intake of AA 1000 mg with a low-fat FDA meal in healthy volunteers resulted in a sevenfold increase in Cmax and a fivefold increase in AUC0–∞ compared to fasted intake. Whereas, with a high-fat FDA meal a 17-fold increase in Cmax and a tenfold increase in AUC0–∞ was seen [7]. Surprisingly, a more modest difference was seen when mCRPC patients ingested 1000 mg AA with a low-fat FDA meal compared to modified fasted intake. The geometric mean ratios (GMRs) fed versus fasted were only 1.35 for Cmax and 1.07 for AUC0–24h [7]. In another study by Attard et al., AA capsules administered with high-fat food in mCRPC patients resulted in a 4.4-fold increased AUC0–∞ [8]. Despite these large differences, the overall picture suggests that AA is much better absorbed in the presence of food. This effect is most likely due to the better solubility of AA in the presence of food, of which the amount of fat in the meal is thought to be the most important [7]. The clinical potential of food to reduce the required dose of AA was shown by Szmulewitz et al. They showed that a reduced dose of 250 mg AA taken with a low-fat breakfast was non-inferior compared to the standard dose of 1000 mg taken fasted for the surrogate endpoint (> 50% PSA response) [9].
Since the effect of food on abiraterone PK is not fully established, a bioequivalence study comparing fasted versus fed intake could contribute to the understanding the effect of food on abiraterone pharmacokinetics. In addition, ingestion of drugs with a breakfast is easier to implement in the patient’s daily life and preferred by most [10]. Consequently, patients are less likely to forget their medication and therefore, an intake regimen with food might positively affect drug adherence.
Therefore, in this study, we aimed to determine the effect of a continental breakfast (CB) on abiraterone exposure and establish the dose reduction required to reach a bio-equivalent exposure compared to the registered intake of 1000 mg OD without food.
Methods
Study design and participants
For this multicentre, phase 1, cross-over study, we enrolled patients from two investigational sites in the Netherlands (Franciscus Gasthuis and Vlietland and Radboud university medical center). Eligible patients were aged 18 or older, had metastatic castration-resistant prostate cancer, were treated with 1000 mg abiraterone acetate (Zytiga®) OD fasted (both patients on treatment and patients who started treatment were eligible) and had an Eastern Cooperative Oncology Group (ECOG) performance status of 0–2 [5]. Patients with gastrointestinal abnormalities that could influence the absorption of AA were excluded. The use of other substances known or likely to interfere with the pharmacokinetics of abiraterone was prohibited during this study.
The trial was approved by the Investigational Review Board of Radboud university medical center, Nijmegen, the Netherlands. The trial was conducted in accordance with Good Clinical Practice and the Declaration of Helsinki and registered at ClinicalTrials.gov, number NCT02883166. All patients gave written informed consent before entering the study.
Procedures
Since the effect of a CB on abiraterone exposure was uncertain and the study was conducted in patients with cancer, a lead-in phase of three patients was introduced. Based on the data of Chi et al., at least a twofold increase in abiraterone exposure taken with food was presumed [7]. Therefore, patients received 500 mg AA with CB. Pharmacokinetic (PK) evaluation after 2 weeks was conducted to prevent unnecessary over- or under-dosing. During the first 2 weeks, patients took 1000 mg AA OD in a fasted state at 08:00 am followed by one of the standardized CBs (Table 1) at 09:00 am. After reaching steady-state pharmacokinetics (day 14), blood was collected in K2-EDTA tubes at t = 0, 1, 2, 3, 4, 5, 6, 8, 10, 12 and 24 h after AA intake for PK assessment. Subsequently, these patients switched to 500 mg AA OD (50% dose reduction) in combination with a standardized CB at 08:00 am. At day 28 of the study, after reaching steady-state pharmacokinetics, the second PK assessment was performed. The results of the first 3 patients were analyzed and evaluated before continuation. If the GMR of the AUC0–24h and Cmax of the reduced dose taken with food compared to the 1000 mg fasted appeared to be within the threshold for bioequivalence (0.8–1.25), the next 21 patients would be exposed to the 50% dose reduction with food. When the 50% dose reducing strategy in the lead-in phase led to a ratio of AUC0–24h and Cmax of more than 1.25, a 75% dose reduction (i.e., 250 mg) would be tested for bioequivalence in a next lead-in of 3 new patients (Fig. 1).

Study design
After each treatment period, patients were asked to complete the validated cancer therapy satisfaction questionnaire (CTSQ) [11]. In the CTSQ, patients are asked about their feelings about side effects, satisfaction with therapy and their expectations of therapy. A difference of ≥ 8.3 points in patients expectations of therapy (ET), ≥ 5.9 point in patients satisfaction with therapy (SWT) and ≥ 10.3 for patients feelings about side effect (FSE) were considered clinically relevant [12].
The CBs were composed by a dietician from Radboudumc and designed to be similar to the breakfasts our patients normally would have. All proposed breakfasts contained the same amount of fat (9–10 g, 25–50% of total caloric intake). The total amount of calories, proteins and carbohydrates differed per breakfast, ranging , respectively, 160–320 Cal, 5–11 g and 15–50 g (Table 1). The choice of CB was at patients’ discretion.
Blood samples for measurement of abiraterone PK were collected on ice and centrifuged within 1 h at 1900g for at least 5 min (4 °C). Plasma samples were stored at − 40 °C until the day of analysis. Abiraterone plasma concentrations were measured using a validated liquid chromatography tandem mass spectrometry method with a range of 1–500 mg/L [13].
Outcomes
The primary endpoint of this study was to determine the equivalent reduced dose of AA when taken with a CB compared to the recommended intake of AA 1000 mg OD taken fasted. Bioequivalence is assumed when the geometric mean ratio (GMR) including the 90% CI of the AUC0–24h, Cmax and Ctrough is within the thresholds of 0.80 and 1.25. Due to the mild toxicity profile of abiraterone (e.g., no treatment-related grade 3 or 4 toxicities occurred at doses twice the registered dose), CI crossing the upper limit of 1.25 is accepted [8].
Statistical analysis
Based on an intra-patient coefficient of variation (CV) of 25%, and a reference ratio of 1.0, a sample size of 24 patients was required for a power of 80%, a two-side significance level of 0.05 and a CV of 20% on the log-transformed data [14]. The AUC0–24h, Cmax, Ctrough, were calculated using non-compartmental analyses in WinNonlin/Phoenix version 6.3 (Pharsight Corporation®). The CTSQ questionnaires were scored following the guideline provided by Abetz et al. [12]. The differences in CTSQ scores were analyzed according to Altman et al. to correct for a possible period effect [15].
Results
Between November 2016 and January 2019, a total of 14 Caucasian patients treated with AA for metastatic castration-resistant prostate cancer were enrolled in the study, of which 12 were evaluable for pharmacokinetic analysis. One patient stopped AA therapy before the second PK evaluation due to elevation in liver enzymes and one patient did not take the medication as prescribed. Both patients were, therefore, excluded from analysis. Of the 12 eligible patients, 10 received prior systemic treatment. Two patients were treatment naïve. Eight patients already used AA before study participation. The median age of the patients was 70 (range 64–93) years (Table 2).
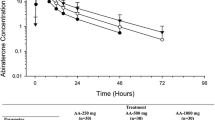
In the initial lead-in phase of the study, three patients were treated with a reduced dose of 500 mg OD with a CB. These three patients showed a geometric mean (GM) AUC0–24h value with and without food of 595 mg h/L and 598 mg h/L, respectively. The GM Cmax values with and without food were 116 mg/L and 115 mg/L, respectively. The GMRs fed/fasted calculated in these patients were 1.01 and 0.99 for AUC0–24h and Cmax. Based on these results, a reduced dose of 50% with a CB was studied in the following patients.
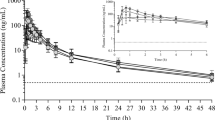
In the final PK analysis in 12 patients, the GM of the AUC0–24h was 776 mg h/L and the Cmax was 148 mg/L, respectively, when 1000 mg abiraterone was taken in a fasted state. When a reduced dose of 500 mg abiraterone was taken with a CB, the GM of the AUC0–24h and the Cmax was 686 mg h/L and 152 mg/L, respectively. The GM of the Ctrough was 10.7 mg/L, when 1000 mg was taken fasted, compared to 8.7 mg/L, when 500 mg was taken with a CB (Fig. 2, Table 3).

Concentration time curve of 1000 mg abiraterone acetate taken fasted and 500 mg abiraterone acetate taken with a continental breakfast
To determine the difference between both intake regimens on AUC0–24h, Cmax and Ctrough the GMRs fed/fasted were calculated including the 90% CI. For AUC0–24h the GMR was 0.88 (90% CI 0.73–1.07), for Cmax the GMR was 1.03 (90% CI 0.79–1.34) and for Ctrough the GMR was 0.81 (90% CI 0.60–1.10). These GMRs with their 90% confidence intervals do not fall within the thresholds predefined for bioequivalence (0.80–1.25) (Fig. 3).

Geometric mean ratio including their confidence interval. Vertical lines represent the threshold of 0.8 and 1.25 as defined by the FDA
Due to the large variation in the individual GMRs observed in our study, we decided after 12 patients that bioequivalence could not be confirmed even when the predefined number of 24 patients would be met. Therefore, further enrolment was stopped.
Inter-patient variability (CV %) for AUC0–24h, Cmax, and Ctrough was 65% vs. 57%, 55% vs. 57% and 72% vs. 75%, respectively, when abiraterone was taken fasted compared to fed.
Compared to 1000 mg taken fasted, patients seem to be slightly more positive about the intake of 500 mg abiraterone with a continental breakfast based on the differences in FSE, SWT and ET fasted versus fed of 2.8, 6.6 and 8.5 points, respectively (Table 4).
Discussion
We aimed to establish the dose reduction required to reach a bioequivalent exposure compared to the standard intake of 1000 mg abiraterone acetate OD without food. Although the GMRs of the intake of 500 mg abiraterone acetate with a continental breakfast compared to 1000 mg taken fasted are within the thresholds of 0.80 and 1.25, the 90% confidence intervals do not meet the criteria for bioequivalence. However, it is known that no exposure–toxicity relation has been found for abiraterone when investigated up until doses of 2000 mg [8]. Therefore, the strict bio-equivalence margins as defined by the FDA guidelines could be applied more flexible for abiraterone.
To the best of our knowledge, this is the first study to investigate the bioequivalence of an adjusted AA dose when taken with food. Our data demonstrated that a 50% dose reduction resulted in a GMR for the AUC0–24h and Ctrough below 1.0. Based on our PK data, no further dose reduction was deemed feasible. However, Szmulewitz et al. have shown that a 75% reduced AA dose taken with a low-fat breakfast resulted in similar PSA response rates compared to the standard fasted intake of AA 1000 mg OD [9]. The descriptive PK data in their study demonstrated that the abiraterone Ctrough levels were lower in the group treated at the reduced dose with food compared to the full dose taken fasted [9]. Nevertheless, despite the lower Ctrough levels, the percentage of patients reaching an adequate PSA response remained comparable between both intake regimes [9]. The majority of the patients in the study of Szmulewitz et al. was treated prior to receiving chemotherapy and might, therefore, be more sensitive to lower abiraterone concentrations. Xu et al. showed that the EC50 of the PSA for abiraterone was 1.56 ng/mL in chemotherapy-naïve patients and 4.75 ng/mL in patients who underwent previous chemotherapy [16]. Though, due to the large confidence intervals around the observation of Xu et al., the data of those trials should be interpreted carefully. Our population mainly consisted of patients post chemotherapy, Therefore, exposure levels similar to those reached when 1000 mg AA taken fasted were aimed for. The results of our study are based on 12 patients instead of the predefined 24 patients. Variation of the individual GMRs of the AUC0–24h and Cmax was larger than expected. Re-estimation of the sample, size based on the larger variability as observed in our study, learned us that bioequivalence could not be demonstrated in the predefined number of 24 patients. Therefore we considered it unethical to further conduct the study. Nevertheless, as 12 patients are the minimal number necessary for a bioequivalence study as stated by the FDA, the PK results from our study are still of value for further interpretation [17]. Since we could not demonstrate bioequivalence, the switch of large groups of patients to an alternative intake regime of 500 mg taken with food cannot be supported. However, because the GMRs of the AUC0–24h, Cmax and Ctrough were within the threshold of 0.8–1.25, the data are suggestive for bioequivalence [18]. Therefore, in individual patients, intake of 500 mg with a CB accompanied with PK monitoring could be considered when experiencing difficulties with a fasted intake.
During our study, patients could choose between seven different types of breakfast. Though standardized for the amount of fat, differences in total caloric intake between the breakfasts were present. This could have enhanced the inter-patient variability. However, our results demonstrate that the inter-patient variability in our study was comparable to other data and was not increased when AA was ingested with food [16, 19]. It, therefore. is not expected that the differences in breakfast contribute to the inter-patient variability.
Our study is the first to explore patient satisfaction when abiraterone is taken with food as a clinical outcome. Our study indicates a modest improvement in treatment satisfaction and expectation of therapy when 500 mg of abiraterone was taken with food. The absence of any notable differences regarding patients feelings about side effects is likely due to the limited gastro-intestinal adverse events such as diarrhea or nausea that patients experience when treated with abiraterone (1–3% grade 3 or 4) [3]. Therefore, ingesting AA with food will not contribute to a reduction of these adverse events.
For several other drugs with this large intra- and inter-patient PK variability, the formulation was adjusted to increase drug absorption and drug exposure to achieve a better predictable response in patients. Examples of drugs with alternative formulations due to absorption issues are regorafenib and olaparib [20, 21]. Also for AA, a new formulation is tested, using a continuous flow precipitation technology. This new formulation shows improved bioavailability, and therefore less PK variability. In addition, food does not play a significant role in the absorption of this new abiraterone formulation [22]. We believe that this new formulation, which is not available yet, could help to overcome the issues of highly variable PK and thereby unpredictable treatment effect for patients.
In conclusion, a bioequivalent lower dose of abiraterone taken with food could not be established in our study. Though, information on the effect of food on abiraterone pharmacokinetics as presented in our study can be used.
References
Kang SP, Ratain MJ (2010) Inconsistent labeling of food effect for oral agents across therapeutic areas: differences between oncology and non-oncology products. Clin Cancer Res 16(17):4446–4451
James ND, de Bono JS, Spears MR, Clarke NW, Mason MD, Dearnaley DP, Ritchie AWS, Amos CL, Gilson C, Jones RJ, Matheson D, Millman R, Attard G, Chowdhury S, Cross WR, Gillessen S, Parker CC, Russell JM, Berthold DR, Brawley C, Adab F, Aung S, Birtle AJ, Bowen J, Brock S, Chakraborti P, Ferguson C, Gale J, Gray E, Hingorani M, Hoskin PJ, Lester JF, Malik ZI, McKinna F, McPhail N, Money-Kyrle J, O’Sullivan J, Parikh O, Protheroe A, Robinson A, Srihari NN, Thomas C, Wagstaff J, Wylie J, Zarkar A, Parmar MKB, Sydes MR, Investigators S (2017) Abiraterone for prostate cancer not previously treated with hormone therapy. N Engl J Med 377:338–351
Fizazi K, Scher HI, Molina A, Logothetis CJ, Chi KN, Jones RJ, Staffurth JN, North S, Vogelzang NJ, Saad F, Mainwaring P, Harland S, Goodman OB Jr, Sternberg CN, Li JH, Kheoh T, Haqq CM, de Bono JS, Investigators C-A (2012) Abiraterone acetate for treatment of metastatic castration-resistant prostate cancer: final overall survival analysis of the COU-AA-301 randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol 13(10):983–992
Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, Ozguroglu M, Ye D, Feyerabend S, Protheroe A, Sulur G, Luna Y, Li S, Mundle S, Chi KN (2019) Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol 20(5):686–700
FDA Abiraterone (Zytigat) product label. http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/202379lbl.pdf. Accessed 20 Sept 2016
FDA (2010) Abirateron (Zytiga) Clinical Pharmacology and Biopharmaceutics review. http://www.accessdata.fda.gov/drugsatfda_docs/nda/2011/202379Orig1s000TOC.cfm. Accessed 21 Mar 2016
Chi KN, Spratlin J, Kollmannsberger C, North S, Pankras C, Gonzalez M, Bernard A, Stieltjes H, Peng L, Jiao J, Acharya M, Kheoh T, Griffin TW, Yu MK, Chien C, Tran NP (2015) Food effects on abiraterone pharmacokinetics in healthy subjects and patients with metastatic castration-resistant prostate cancer. J Clin Pharmacol 55(12):1406–1414
Attard G, Reid AH, Yap TA, Raynaud F, Dowsett M, Settatree S, Barrett M, Parker C, Martins V, Folkerd E, Clark J, Cooper CS, Kaye SB, Dearnaley D, Lee G, de Bono JS (2008) Phase I clinical trial of a selective inhibitor of CYP17, abiraterone acetate, confirms that castration-resistant prostate cancer commonly remains hormone driven. J Clin Oncol 26(28):4563–4571
Szmulewitz RZ, Peer CJ, Ibraheem A, Martinez E, Kozloff MF, Carthon B, Harvey RD, Fishkin P, Yong WP, Chiong E, Nabhan C, Karrison T, Figg WD, Stadler WM, Ratain MJ (2018) Prospective international randomized phase II study of low-dose abiraterone with food versus standard dose abiraterone in castration-resistant prostate cancer. J Clin Oncol 36:1389–1395
Lubberman F (2019) A reduced pazopanib dose with food: is it more patient-friendly and does it reduce drug costs? J Clin Oncol 37(suppl):abstr 4564
Trask PC, Tellefsen C, Espindle D, Getter C, Hsu MA (2008) Psychometric validation of the cancer therapy satisfaction questionnaire. Value Health 11(4):669–679
Abetz L, Coombs JH, Keininger DL, Earle CC, Wade C, Bury-Maynard D, Copley-Merriman K, Hsu MA (2005) Development of the cancer therapy satisfaction questionnaire: item generation and content validity testing. Value Health 8(Suppl 1):S41–S53
Benoist GE, van der Meulen E, Lubberman FJE, Gerritsen WR, Smilde TJ, Schalken JA, Beumer JH, Burger DM, van Erp NP (2017) Analytical challenges in quantifying abiraterone with LC-MS/MS in human plasma. Biomed Chromatogr 31(11):e3986
Diletti E, Hauschke D, Steinijans VW (1991) Sample size determination for bioequivalence assessment by means of confidence intervals. Int J Clin Pharmacol Ther Toxicol 29(1):1–8
Altman DG (1991) Practical statistics for medical Research, 1st edn. Chapman & Hall, London
Xu XS, Ryan CJ, Stuyckens K, Smith MR, Saad F, Griffin TW, Park YC, Yu MK, De Porre P, Vermeulen A, Poggesi I, Nandy P (2017) Modeling the relationship between exposure to abiraterone and prostate-specific antigen dynamics in patients with metastatic castration-resistant prostate cancer. Clin Pharmacokinet 56(1):55–63
FDA (2002) Guidance for industry bioavailability and bioequivalence studies for orally administered drug products—general considerations. http://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/AbbreviatedNewDrugApplicationANDAGenerics/UCM154838.pdf. Accessed 21 Mar 2016
Williams RL, Chen ML, Hauck WW (2002) Equivalence approaches. Clin Pharmacol Ther 72(3):229–237
Arasaratnam M, Crumbaker M, Bhatnagar A, McKay MJ, Molloy MP, Gurney H (2019) Inter- and intra-patient variability in pharmacokinetics of abiraterone acetate in metastatic prostate cancer. Cancer Chemother Pharmacol 84:139–146
FDA Regorafenib clinical pharmacology and biopharmaceutics review. https://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/203085Orig1s000ClinPharmR.pdf. Accessed 22 Jan 2019
Mateo J, Moreno V, Gupta A, Kaye SB, Dean E, Middleton MR, Friedlander M, Gourley C, Plummer R, Rustin G, Sessa C, Leunen K, Ledermann J, Swaisland H, Fielding A, Bannister W, Nicum S, Molife LR (2016) An adaptive study to determine the optimal dose of the tablet formulation of the PARP inhibitor olaparib. Target Oncol 11(3):401–415
Solymosi T, Otvos Z, Angi R, Ordasi B, Jordan T, Molnar L, McDermott J, Zann V, Church A, Mair S, Filipcsei G, Heltovics G, Glavinas H (2017) Novel formulation of abiraterone acetate might allow significant dose reduction and eliminates substantial positive food effect. Cancer Chemother Pharmacol 80(4):723–728
Acknowledgements
We thank patients and their families, all investigators, research nurses: A. Hofboer, K. Saini and S. Ras, dietician: Heidi Zweers who designed the breakfasts used in the study; and ‘Betaalbaar Beter’ for the financial support.
Funding
This study was supported by the health insurance company VGZ within the program ‘Betaalbaar Beter’.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
NvE received grants from Novartis, Astellas, AstraZeneca, Bristol-Meyers Squibb, Gilead, Ipsen, Janssen, Pfizer and Roche. IvO received grants from Astellas, Janssen, Sanofi, Beyer and Roche. The other authors declare to have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Lubberman, F.J.E., Benoist, G.E., Gerritsen, W. et al. A prospective phase I multicentre randomized cross-over pharmacokinetic study to determine the effect of food on abiraterone pharmacokinetics. Cancer Chemother Pharmacol 84, 1179–1185 (2019). https://doi.org/10.1007/s00280-019-03952-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-019-03952-w