
Abstract
Purpose
Systemic chemotherapy is the treatment of choice for AIDS-related advanced Kaposi sarcoma. One principal schedule combines adriamycin (doxorubicin), bleomycin, and vincristine (ABV). We analysed the plasma concentrations of low-dose doxorubicin (Dx) and its metabolites doxorubicinol, 7-deoxydoxorubicinone, doxorubicinone, doxorubicinolone, and 7-deoxydoxorubicinolone in AIDS-patients to define patient-group and dose-specific pharmacokinetic parameters.
Materials and methods
A previously described high-performance liquid chromatographic (HPLC) method and a population approach with non-linear mixed effects modelling (NONMEM) were used for analysis and subsequent modelling of the time–concentration data of low-dose Dx and metabolites in seven patients with AIDS-related advanced Kaposi sarcoma. Patients received Dx 20 mg m−2, bleomycin 15 U m−2 and vincristine 2 mg as a 30-min intravenous infusion each. Blood samples were collected up to 72 h after the start of Dx treatment. WinNonlin software version 4.1 was used for non-compartmental analysis and NONMEM software version V for compartmental analysis. Covariate analysis was performed for various clinical and laboratory parameters.
Results
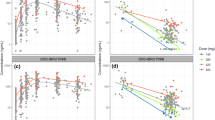
Non-compartmental analysis yielded an area under the plasma concentration–time curve (AUC) for Dx of 566 μg h L−1, a maximum plasma concentration (cmax) of 599 μg L−1 and an elimination half-life (t1/2) of 30.8 h. Compartmental analysis resulted in a two-compartment model with first-order elimination, which best fitted the concentration–time data. Model estimate for Dx clearance was 61.8 L h−1, for intercompartmental clearance (Q) 112 L h−1, for the volume of the central compartment (V1) 23.3 L, and for the volume of the peripheral compartment (V2) 1,130 L. Metabolite data could adequately be estimated by NONMEM using single-compartment models. Graphical plots of residuals versus time for all metabolites yielded no evidence of non-linear pharmacokinetic behaviour. Laboratory parameters of liver and renal function were all in the normal range and their inclusion in the pharmacokinetic model did not improve data fit. A final jack-knife analysis was performed.
Conclusions
Concentration–time data for low-dose Dx and metabolites in the ABV-regimen are best described by a two-compartment model with first-order elimination. The results confirm that the aglycones doxorubicinone, 7-deoxydoxorubicinone, and doxorubicinolone can be reliably detected in the studied patient group and implemented into a common metabolic model. Model estimates suggest that pharmacokinetic parameters are similar for low-dose Dx and higher-dosed Dx. As the role of the aglycones is still poorly understood, despite their potential clinical relevance, their analysis should be implemented in future pharmacokinetic and pharmacodynamic studies of Dx.




Similar content being viewed by others


References
Mitsuyasu RT (2000) Update on the pathogenesis and treatment of Kaposi sarcoma. Curr Opin Oncol 12:174–180
Von Roenn JH, Krown SE (1998) Management of AIDS-associated Kaposi’s sarcoma: a multidisciplinary perspective. Oncology (Huntingt) 12:1–24
Robert J (1998) Anthracyclines. In: Grochow LB, Ames MM (eds) A clinician’s guide to chemotherapy pharmacokinetics and pharmacodynamics. Williams&Wilkins, Baltimore, pp 93–173
Bouma J, Beijnen JH, Bult A, Underberg WJ (1986) Anthracycline antitumour agents. A review of physicochemical, analytical and stability properties. Pharm Weekbl Sci 8:109–133
Cummings J, Merry S, Willmott N (1986) Disposition kinetics of adriamycin, adriamycinol and their 7-deoxyaglycones in AKR mice bearing a sub-cutaneously growing ridgway osteogenic sarcoma (ROS). Eur J Cancer Clin Oncol 22:451–460
Andersen A, Holte H, Slordal L (1999) Pharmacokinetics and metabolism of doxorubicin after short-term infusions in lymphoma patients. Cancer Chemother Pharmacol 44:422–426
Piscitelli SC, Rodvold KA, Rushing DA, Tewksbury DA (1993) Pharmacokinetics and pharmacodynamics of doxorubicin in patients with small cell lung cancer. Clin Pharmacol Ther 53:555–561
Mross K, Maessen P, van der Vijgh WJF, Gall H, Boven E, Pinedo HM (1988) Pharmacokinetics and metabolism of epidoxorubicin and doxorubicin in humans. J Clin Oncol 6:517–526
Frenay M, Milano G, Renee N, Pons D, Khater R, Francois E, Thyss A, Namer M (1989) Pharmacokinetics of weekly low dose doxorubicin. Eur J Cancer Clin Oncol 25:191–195
Speth PA, Linssen PC, Holdrinet RS, Haanen C (1987) Plasma and cellular adriamycin concentrations in patients with myeloma treated with ninety-six-hour continuous infusion. Clin Pharmacol Ther 41:661–665
Robert J, Gianni L (1993) Pharmacokinetics and metabolism of anthracyclines. Cancer Surv 17:219–252
Eksborg S, Strandler HS, Edsmyr F, Naslund I, Tahvanainen P (1985) Pharmacokinetic study of i.v. infusions of adriamycin. Eur J Clin Pharmacol 28:205–212
Licata S, Saponiero A, Mordente A, Minotti G (2000) Doxorubicin metabolism and toxicity in human myocardium: role of cytoplasmic deglycosidation and carbonyl reduction. Chem Res Toxicol 13:414–420
Beijnen JH, Meenhorst PL, van Gijn R, Fromme M, Rosing H, Underberg WJM (1991) HPLC determination of doxorubicin, doxorubicinol and four aglycone metabolites in plasma of AIDS patients. J Pharm Biomed Anal 9:995–1002
Beal SL, Sheiner LB (1998) NONMEM User’s Guide University of California at San Francisco: NONMEM Project Group
Jonsson EN, Karlsson MO (1999) Xpose—an S-PLUS based population pharmacokinetic/pharmacodynamic model building aid for NONMEM. Comput Methods Programs Biomed 58:51–64
Cummings J, Milstead R, Cunningham D, Kaye S (1986) Marked inter-patient variation in adriamycin biotransformation to 7-deoxyaglycones: evidence from metabolites identified in serum. Eur J Cancer Clin Oncol 22:991–1001
Levine AM, Tulpule A, Espina B, Boswell W, Buckley J, Rasheed S, Stain S, Parker J, Nathwani B, Gill PS (1996) Low dose methotrexate, bleomycin, doxorubicin, cyclophosphamide, vincristine, and dexamethasone with zalcitabine in patients with acquired immunodeficiency syndrome-related lymphoma. Effect on human immunodeficiency virus and serum interleukin-6 levels over time. Cancer 78:517–526
Chlebowski RT, Paroly WS, Pugh RP, Hueser J, Jacobs EM, Pajak TF, Bateman JR (1980) Adriamycin given as a weekly schedule without a loading course: clinically effective with reduced incidence of cardiotoxicity. Cancer Treat Rep 64:47–51
Mattsson W, Borgstrom S, Landberg T (1982) A weekly schedule of low-dose doxorubicin in treatment of advanced breast cancer. Clin Ther 5:193–203
Torti FM, Bristow MR, Howes AE, Aston D, Stockdale FE, Carter SK, Kohler M, Brown BW Jr, Billingham ME (1983) Reduced cardiotoxicity of doxorubicin delivered on a weekly schedule. Assessment by endomyocardial biopsy. Ann Intern Med 99:745–749
Speth PA, van Hoesel QG, Haanen C (1988) Clinical pharmacokinetics of doxorubicin. Clin Pharmacokinet 15:15–31
Rudek MA, Sparreboom A, Garrett-Mayer ES, Armstrong DK, Wolff AC, Verweij J, Baker SD (2004) Factors affecting pharmacokinetic variability following doxorubicin and docetaxel-based therapy. Eur J Cancer 40:1170–1178
Acknowledgements
M. Joerger is supported by a Novartis-UICC Translational Cancer Research Fellowship funded by Novartis AG and by a research grant from the Swiss National Science Foundation (PBBSB-102331).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Joerger, M., Huitema, A.D.R., Meenhorst, P.L. et al. Pharmacokinetics of low-dose doxorubicin and metabolites in patients with AIDS-related Kaposi sarcoma. Cancer Chemother Pharmacol 55, 488–496 (2005). https://doi.org/10.1007/s00280-004-0900-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-004-0900-4