
Abstract
Introduction
Covid-19 has had a significant impact on all aspects of health care. We aimed to characterise the trends in emergency general surgery at a district general hospital in Scotland.
Methods
A prospective cohort study was performed from 23/03/20 to 07/05/20. All emergency general surgery patients were included. Demographics, diagnosis and management were recorded along with Covid-19 testing and results. Thirty-day mortality and readmission rates were also noted. Similar data were collected on patients admitted during the same period in 2019 to allow for comparison.
Results
A total of 294 patients were included. There was a 58.3 per cent reduction in admissions when comparing 2020 with 2019 (85 vs 209); however, there was no difference in age (53.2 vs 57.2 years, p = 0.169) or length of stay (4.8 vs 3.7 days, p = 0.133). During 2020, the diagnosis of appendicitis increased (4.3 vs 18.8 per cent, p = < 0.05) as did severity (0 per cent > grade 1 vs 58.3 per cent > grade 1, p = < 0.05). The proportion of patients undergoing surgery increased (19.1 vs 42.3 per cent, p = < 0.05) as did the mean operating time (102.4 vs 145.7 min, p = < 0.05). Surgery was performed in 1 confirmed and 1 suspected Covid-19 patient. The latter died within 30 days. There were no 30-day readmissions with Covid-19 symptoms.
Conclusion
Covid-19 has significantly impacted the number of admissions to emergency general surgery. However, emergency operating continues to be needed at pre-Covid-19 levels and as such provisions need to be made to facilitate this.
Similar content being viewed by others


Introduction
Since first presenting in late 2019 [1], the effect of Covid-19 has been worldwide. Primarily affecting the respiratory system [2], the burden on health care has been profound [3]. Whilst a significant proportion of this is directly disease related, the secondary impact on health is yet to be determined but will likely influence the overall effect this pandemic has on our society [4]. In particular, the delivery of surgical services has been dramatically compromised [5] with cancellation of all but essential surgery in Scotland [6]. Not only does this free up valuable resources but the mortality associated with surgery in a Covid-19 positive patient is reported to be as high as 20.5% [7]. In addition, many aspects of surgery are considered to be aerosol generating, and therefore, health care workers are at potential risk should necessary precautions not be taken [8]. In response to this, the United Kingdom Intercollegiate guidance was published in late March and outlined recommendations for provision of surgery [9]. It concluded that laparoscopic surgery, given its potential for aerosol generation, should be considered only in selected individuals where clinical benefit exceeds the potential risk of viral transmission. Furthermore, non-operative management of certain conditions was favoured and an open approach for acute appendicitis suggested as a suitable alternative.
Given the strong government message for the public to remain at home, it is unsurprising that this has correlated with a reduction in non-Covid-19 health care use. Most notably, Emergency Department attendances in Scotland dropped by 21.1% during March 2020 [10]. However, it is unclear how acute surgical admissions have changed in response to the pandemic. We aimed to characterise the experience of emergency general surgery in a district general hospital in Scotland and the changes seen compared with the same period in 2019.
Methods
All general surgical emergency admissions to a Scottish, medium-sized, district general hospital were included from 23/03/20 to 07/05/20. The hospital covers a population of approximately 116,000 and provides all general surgical specialties. A tertiary centre is located 30 miles away and provides support for major trauma and complex cases. Patients undergoing a general surgical procedure but under the care of another specialty were also included. After registering with the hospital governance department, inpatient admissions were captured using a data collection form which was completed prospectively by the authors. Patient demographics were noted as was the Covid-19 status at admission. Patients were considered negative if they were admitted to the general surgical ward, unconfirmed if they went to a designated Covid-19 assessment unit but then had a negative test and positive if they had undergone positive testing. The diagnosis and subsequent management were recorded. Of those undergoing surgery, operation notes and histopathology, if applicable, were analysed to determine intra- and post-operative findings. For acute appendicitis, severity was recorded using the disease severity score described by Garst et al. [11] (Table 1).
Particular attention was paid to whether there was an alteration in either the procedure or approach due to Covid-19. It was also noted if a patient was managed conservatively when otherwise would have undergone surgical intervention. Length of stay and 30-day outcomes were then recorded. The 30-day outcomes were all-cause mortality and readmission, either with the same symptoms as the primary admission or with Covid-19 specific symptoms.
Similar data were then collected on patients admitted during the same period in 2019 (23/03/2019–07/05/2019). Patients were identified from the local coding department. This allowed for comparison of demographics, diagnoses, management and outcomes.
Statistical analysis
Continuous variables are presented as mean (S.D.) and categorical variables as number with percentages. Student’s t test and Chi-squared test were used to calculate significance for continuous and categorical variables, respectively. A p value < 0.05 was considered to be statistically significant. All statistical analysis was performed using Microsoft Excel® version 16.35 (Microsoft, Redmond, Washington, USA).
Results
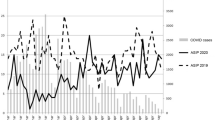
A total of 294 patients were identified in total, 209 in 2019 and 85 during 2020. This represented a 59.3 per cent reduction in emergency admissions. Patient and admission characteristics are shown in Table 2. Covid status and testing are shown in Table 3.
Of the 36 patients undergoing surgery during 2020, 5 (13.9 per cent) had a change in the surgical procedure. These were all appendicectomies which were performed open instead of laparoscopically. Ten (11.8 per cent) patients who would otherwise have been managed surgically had a conservative approach. This included 5 diagnostic laparoscopies (4 radiologically confirmed appendicitis), 4 laparoscopic cholecystectomies and 1 umbilical hernia repair.
One patient died following surgery for ischaemic small bowel and was considered to have a false negative Covid-19 test. The other mortality was not Covid-19 related. There were no readmissions with Covid-19 symptoms.
Discussion
Our results demonstrate the changing trends in emergency general surgery during Covid-19. With overall emergency admissions to hospital falling by 23 and 38.5 per cent during March and April 2020, respectively [12, 13], it is unsurprising that we found an even greater reduction in emergency surgical admissions when compared with the same period in 2019. Although we did not include transfers to tertiary care from the Emergency Department in either cohort, given the breadth of specialties provided in our hospital it is unlikely that there was a significant change in the number of patients requiring immediate transfer. Although there was a decrease in the number of admissions, there was no change seen in patient demographics. With vulnerable patient groups, such as those with significant co-morbidities, being advised to shield [14], a reduction in age could be hypothesised as the former avoid presentation to secondary care. Whilst patients during Covid-19 were younger (53.2 vs 57.2 years), this did not reach a level of statistical significance. The strong public promotion for patients to attend hospital if acutely unwell, regardless of the cause, is likely to have resulted in elderly patients continuing to seek secondary care services.
In addition, we found no difference in either gender of length of hospital stay. Although the gender and length of stay have been described in the literature for patients with Covid-19 [15, 16], little is known about remaining patients during the pandemic. It could be expected that length of stay shortens as hospitals try to increase bed capacity and there is clinical concern about spread of infection. However, we observed an increase in length of stay (3.74 vs 4.84 days, p = 0.133) albeit without statistical significance. This could be attributed to the fact that we saw a decrease in patients with non-specific abdominal pain, a group who often can be discharged following normal investigations and improvement in symptoms [17] and continued to have admissions of patients requiring surgical intervention. Certainly, the proportion of patients requiring an operation increased (19.1 vs 42.4 per cent, p = 0.05) and this may be reflected in the increased mean length of stay. Interestingly, our continuation of emergency surgery is in contrast with that reported elsewhere [18]. However, these data come from regions with a greater outbreak than ours, and therefore, it is likely that there was a greater strain on services.
One of the main differences we identify is in the diagnoses. In particular, there was a significant increase in the number of appendicitis cases (4.3 vs 18.8 per cent, p = < 0.05). Whilst the increase in percentage point is partly attributable to the overall reduction in patient numbers, there was an increase seen in the raw number of cases. Although it is difficult to attribute causal relationship as only 1 of our 16 appendicitis diagnoses had confirmed Covid-19 disease, it has been reported that Covid-19 may present with abdominal pain [19] and it is recognised that it can present with gastrointestinal symptoms only [20]. Furthermore, in our cohort, only 50 per cent of patients diagnosed with acute appendicitis underwent Covid-19 testing. It is therefore possible that there may have been patients with occult infection. Interestingly, we found an increase in the severity of appendicitis at operation. With more patients found to have perforated appendicitis at operation or on histology, it may be that there is an element of delayed presentation. Furthermore, 12 (75 per cent) patients were deemed to require surgical management as opposed to the intercollegiate recommendation of a conservative approach [9] again suggesting an increase in severity. Given its prominence within the intercollegiate guidelines, it is unsurprising that acute appendicitis in itself will be the focus of a multi-centre cohort study [21].
It is also difficult to quantify objectively the technical complexity involved with other procedures. Whilst we did see a statistically significant increase in the mean operating time (102.4 vs 145.7, p = < 0.05), it is unlikely to be attributable to active operating alone. Substantial changes to the operating environment, similar to that described elsewhere [22], and unfamiliarity with this are also likely to contribute to an increase in the operative time.
In accordance with the intercollegiate recommendations, we managed patients non-operatively where possible. This was most relevant to those with acute appendicitis or cholecystitis. In each case, it was discussed with the patient that given the potential risks of surgery, conservative management with antibiotics would be the first line. No patient required surgery or interventional radiology following failed conservative management. Although our number of appendicitis cases is low, it would appear that our experience is comparable to larger cohorts in that there is an acceptable rate of treatment failure [23]. Of course, the longer-term effects remain to be assessed and there will undoubtedly be cases of recurrent appendicitis. With regard to cholecystitis, there remains to be reporting of short-term outcomes of a non-operative approach.
We demonstrate that the majority of emergency general surgical patients did not undergo Covid-19 testing; however, this may be due to initial limitations of testing. The guidance for testing is well published [24]; however, challenges can still present, particularly if there are Covid-19 symptoms which could be attributed to other pathology (e.g. acute appendicitis). Whilst mass testing has been advocated [25], there remain concerns over sensitivity [26] and cost of testing also needs to be considered [27]. Furthermore, our cohort only had 1 patient with a positive Covid-19 test with 1 considered to be a false negative and so our detection rate was low. Equally, undergoing surgery with concurrent Covid-19 infection is associated with a high intensive care unit (ICU) admission and mortality [7], and therefore, frameworks for testing, particularly in those due to undergo elective surgery, are being developed [28]. The two aforementioned patients both underwent surgery and required ICU admission. One required a laparotomy followed by appendicectomy and the other underwent a diagnostic laparotomy which confirmed ischaemic bowel and was deemed not survivable. Although not large in numbers, our experience of surgery in Covid-19 patients is comparable with the literature [7].
Conclusion
Covid-19 has significantly impacted the number of admissions to emergency general surgery. However, emergency operating continues to be needed at pre-Covid-19 levels and as such provisions need to be made to facilitate this.
References
Lai C-C, Wang C-Y, Wang Y-H, Hsueh S-C, Ko W-C, Hsueh P-R (2019) Global epidemiology of coronavirus disease 2019 (COVID-19): disease incidence, daily cumulative index, mortality, and their association with country healthcare resources and economic status. Int J Antimicrob Agents 55(4):105946
Guan W, Ni Z, Hu Y, Liang W, Ou C, He J et al (2019) Clinical characteristics of coronavirus disease 2019, in China. N Engl J Med 382(18):1708–1720
Peters A, Vetter P, Guitart C, Lotfinejad N, Pittet D (2020) Understanding the emerging coronavirus: what it means for health security and infection prevention. J Hosp Infect 104(4):440–448
Tan W, Aboulhosn J (2019) The cardiovascular burden of coronavirus disease, 2019 (COVID-19) with a focus on congenital heart disease. Int J Cardiol 309:70–77
Søreide K, Hallet J, Matthews JB, Schnitzbauer AA, Line PD, Lai PBS et al (2020) Immediate and long-term impact of the COVID-19 pandemic on delivery of surgical services. Br J Surg. https://doi.org/10.1002/bjs.11670
Public Health Scotland (2020) Cancelled Planned Operations March 2020. Public Health Scotland. [Accessed 10 July 2020]. Available from: https://beta.isdscotland.org/find-publications-and-data/healthcare-resources/waiting-times/cancelled-planned-operations/5-may-2020/
Lei S, Jiang F, Xia Z-Y, Xia Z (2020) Author’s reply—clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID-19 infection. EClinicalMedicine 21:100363
Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J (2012) Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS ONE 7(4):35797
Brücher BLDM, Nigri G, Tinelli A, Lapeña JFF, Espin-Basany E, Macri P et al (2020) COVID-19: pandemic surgery guidance. 4open 3:1
Public Health Scotland. A&E activity and waiting times. Public Health Scotland. [Accessed 10 July 2020]. Available from: https://beta.isdscotland.org/find-publications-and-data/health-services/hospital-care/ae-activity-and-waiting-times/5-may-2020/
Garst GC, Moore EE, Banerjee MN, Leopold DK, Burlew CC, Bensard DD et al (2013) Acute appendicitis. J Trauma Acute Care Surg 74(1):32–36
Appleby J (2020) What is happening to non-covid deaths? BMJ 369:m1607
NHS England. Monthly Hospital Activity Data. NHS England. [Accessed 10 July 2020]. Available from: https://www.england.nhs.uk/statistics/statistical-work-areas/hospital-activity/monthly-hospital-activity/mar-data/
Smith GD, Spiegelhalter D (2020) Shielding from covid-19 should be stratified by risk. BMJ 369:m2063
Jin J-M, Bai P, He W, Wu F, Liu X-F, Han D-M et al (2020) Gender differences in patients with COVID-19: focus on severity and mortality. Front Public Health 8:152
Rees EM, Nightingale ES, Jafari Y, Waterlow N, Clifford S, Group CW, et al. (2020) COVID-19 length of hospital stay: a systematic review and data synthesis. medRxiv. 2020.04.30.20084780
Sheridan WG, White AT, Havard T, Crosby DL, De Dombal FT (1992) Non-specific abdominal pain: the resource implications. Ann R Coll Surg Engl 74(3):181–185
Patriti A, Eugeni E, Guerra F (2020) What happened to surgical emergencies in the era of COVID-19 outbreak? Considerations of surgeons working in an Italian COVID-19 red zone. Updates Surg 72(2):309–310
Saeed U, Sellevoll HB, Young VS, Sandbaek G, Glomsaker T, Mala T (2020) Covid-19 may present with acute abdominal pain. Br J Surg 107(7):e186–187
Poggiali E, Ramos PM, Bastoni D, Vercelli A, Magnacavallo A (2020) Abdominal pain: a real challenge in novel COVID-19 infection. Eur J Case Rep Intern Med 7(4):001632
Javanmard-Emamghissi H, Hollyman M, Daliya P, Adiamah A, Pearce L, Cornish J et al (2020) The HAREM (Had appendicitis and resolved/recurred emergency morbidity/mortality) study. Br J Surg 107(8):e257–e257
Tan Z, Phoon PHY, Zeng LA, Fu J, Lim XT, Tan TE et al (2020) Response and operating room preparation for the COVID-19 outbreak: a perspective from the national heart centre in Singapore. J Cardiothorac Vasc Anesth 34(9):2331–2337
Javanmard-Emamghissi H, Boyd-Carson H, Hollyman M, Doleman B, Adiamah A, Lund JN et al (2020) The management of adult appendicitis during the COVID-19 pandemic: an interim analysis of a UK cohort study. Tech Coloproctol. https://doi.org/10.1007/s10151-020-02297-4
Beeching NJ, Fletcher TE, Beadsworth MBJ (2020) Covid-19: testing times. BMJ 369:m1403
Peto J (2020) Covid-19 mass testing facilities could end the epidemic rapidly. BMJ. m1163
Zitek T (2020) The appropriate use of testing for COVID-19. West J Emerg Med 21(3):470–472
Mark K, Steel K, Stevenson J, Evans C, McCormick D, Willocks L, et al. (2020) Coronavirus disease (COVID-19) community testing team in Scotland: A 14-day review, 6 to 20 February 2020. Eurosurveillance 25(12)
Al-Muharraqi MA (2020) Testing recommendation for COVID-19 (SARS-CoV-2) in patients planned for surgery - continuing the service and ‘suppressing’ the pandemic. Br J Oral Maxillofac Surg 58(5):503–505
Funding
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declared that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dick, L., Green, J., Brown, J. et al. Changes in Emergency General Surgery During Covid-19 in Scotland: A Prospective Cohort Study. World J Surg 44, 3590–3594 (2020). https://doi.org/10.1007/s00268-020-05760-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-020-05760-3