
Abstract
Background
For both gallbladder removal and inguinal hernia repair, it is important to include patients’ perspective in the decision-making process, as watchful waiting is an accepted alternative in selected patients. The aim of this study was to evaluate operation rates before and after implementation of decision aids (DAs) and to assess patient compliance with the use of DAs.
Methods
A single-centered retrospective study was performed, including all patients ≥18 years referred to the surgical outpatient clinic with symptomatic gallstones or an inguinal hernia between January 2014 and December 2017. Operation rates before and after implementation of DAs (December 2015) were compared. In addition, patient compliance with the use of DAs and satisfaction with final treatment were assessed.
Results
Overall, 1625 patients with gallstones and 1798 patients with an inguinal hernia were included. After implementation, DAs were provided to 512 patients (63.1%) with gallstones of whom 80.7% (413/512) used the DA and to 528 patients (58.8%) with an inguinal hernia, which was used by 80.7% (426/528). Before implementation, the operation rate in patients with gallstones was 72.0% (586/814) and after implementation 56.7% (460/811) (− 15.3%, p < 0.001). The operation rate in patients with an inguinal hernia decreased from 77.8% (700/900) to 64.6% (580/898) (− 13.2%, p < 0.001). Patient satisfaction with final treatment was high (9/10).
Conclusion
Implementation of DAs in the surgical outpatient clinic for patients with gallstones or an inguinal hernia is associated with reduced elective operation rates and is associated with high DA compliance.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gallbladder removal and inguinal hernia repair are the two most commonly performed surgical procedures worldwide [1, 2]. Both procedures are mostly elective and straightforward procedures with relatively low surgical risks [3,4,5,6]. For both operations, watchful waiting is an accepted alternative in patients with uncomplicated disease [7,8,9,10]. Although a conservative treatment is less practiced, this strategy is associated with relatively low rates of complications [11,12,13,14].
Patients consider it crucial to be involved in the decision making for treatments [15]. Shared decision making (SDM) as a model for treatment decisions balances patient’s preferences, medical expertise of the doctor and clinical evidence from trials [16]. In this way, SDM counterbalances the dominance of the physician’s perspective [16,17,18]. A recent study shows the growing international interest of SDM in surgery [19]. SDM can be facilitated by decision aids (DAs), i.e., tools with balanced, patient-adjusted information about the harms and benefits of treatments [20, 21]. A systematic review of 105 randomized controlled trials on DAs provides evidence for more knowledgeable patients who are more clear about their values after the use of a DA [20]. DAs for different kinds of surgeries increase patient involvement and decrease decisional conflict; moreover, patients chose more frequently conservative or less-invasive treatment options [22]. However, the impact of DAs on surgical rates in general surgical practice is unreported.
Based on the literature on other surgical procedures, we hypothesized that operation rates might decrease after implementation of DAs. Therefore, the aim of this study was firstly to determine the impact of the implementation of DAs comparing surgery with watchful waiting on the operation rates. Secondly, we assessed the compliance with the use of DAs in patients. Finally, we evaluated patient satisfaction with final treatment and persistent pain after the decision for either surgery or watchful waiting was made, as a measure for clinical efficacy.
Methods
Study design and study population
A single-centered retrospective study was performed in a general hospital in the Netherlands. All patients, 18 years or older, with a new referral to the surgical outpatient clinic and with symptomatic gallstones or an inguinal hernia who attended the clinic between January 2014 and December 2017 were included. All patients with an emergency operation were excluded; 320 patients with gallstones (140 patients before implementation and 180 patients after implementation) and 47 emergency patients with an inguinal hernia were excluded (26 before implementation and 21 after). In general, Dutch patients are diagnosed with gallstones or an inguinal hernia by their general practitioner and are then referred for treatment advice to the local hospital. In our hospital, online DAs providing detailed information about surgery and watchful waiting are part of standard care in the surgical outpatient clinic for patients with gallstones or an inguinal hernia since December 2015.
The local medical ethical committee and the boards of directors reviewed and approved the study protocol (registration number 2017-3973). This research was performed in accordance with the ethical standards of the Helsinki Declaration of 1975. All included patients for secondary analyses gave written informed consent. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines were followed [23].
Outcome and data collection
Primary outcome of this study was the difference in operation rate before and after implementation of DAs for gallstones and inguinal hernia in all patients with a new referral to the surgical outpatient clinic. Patients were identified based on diagnosis-related groups (DRG’s). Data regarding the operation were collected from the electronic hospital registry. As the DRG’s for both gallstones and inguinal hernia patients do not discriminate complicated disease profiles from noncomplicated conditions (e.g., cholecystitis and non-reducible hernia) in the Dutch system, no distinction between patients with complicated and uncomplicated disease could be made.
Secondary outcome was patient compliance with the use of DAs, which was assessed in patients included from December 2015 onwards. Compliance was defined as use of a DA by patients, assessed by answers on all questions in step 3, 4 and 5 of the DA. Three groups of patients could be identified: 1) patients who did not receive a DA (total patients minus patients who received a DA), 2) patients who received a DA but did not use it and 3) patients who received a DA and used it.
Satisfaction with final treatment and persistent pain were assessed in a subgroup of patients who used the DA and attended the outpatient clinic between January 2017 and September 2017. The survey and informed consent form were sent in April 2018. This subgroup was chosen to prevent recall bias and to acquire sufficient adequate follow-up. The survey consisted of questions on patient characteristics, treatment and two additional questions (How satisfied are you with the final treatment? Do you still experience pain?). Both questions were answered on a scale from 0 to 10. The questionnaires were sent by mail, and a reminder was sent by email to patients who did not respond after 4 weeks. Patients who had not responded after another 4 weeks were reminded by phone. The referral pattern to the outpatient clinic (e.g., emergency room, general practitioner or internal medicine) was depicted from the electronic patient record in patients who gave informed consent.
Decision aids
The online DAs were developed by patients and physicians according to the International Patient Decision Aids Standards (IPDAS) and comprise five steps. More information about the development and implementation of the DA is given in “Appendix.”
Statistical analysis
Continuous data were presented as mean with standard deviation when normally distributed and median with range or inter-quartile range when non-normally distributed. Dichotomous data were summarized by frequencies and proportions. The operation rates before and after implementation were calculated by dividing the number of operated patients by the total number of new referrals to the outpatient clinic of surgery. The primary outcome, i.e., the difference in operation rates, was analyzed using Chi-squared test. Compliance with the use of DAs was calculated by dividing the patients that received a DA by the total patients and secondly by dividing the patients that used the DA by the patients that received a DA.
Nonresponse analyses were performed for the responders and nonresponders to the questionnaire for sex, age and performed treatment. Within the responders, patients with an operative and nonoperative treatment were compared by sex, age, BMI, and long-term satisfaction and persistent pain. Pain-free was defined as a pain score equal to or lower than 4 [24, 25]. Responders with gallstones were compared by referral pattern, and responders with an inguinal hernia were compared by side of hernia. Comparison of clinical characteristics between both groups was done using the Chi-squared test for dichotomous data, the Student’s t test for normally distributed continuous data and the Mann–Whitney U test for skewed continuous data.
Associations with a p value less than 0.05 will be considered statistically significant. All missing values were considered to be at random and were excluded from the analyses. Analyses were performed using SPSS statistics version 22.0 (IBM).
Results
Patients
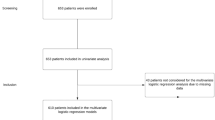
Between January 2014 and December 2017, 1625 patients with gallstones and 1798 patients with an inguinal hernia were included; in these patients, operation rates were assessed (Fig. 1). A total of 180 gallstone patients and 21 inguinal hernia patients were excluded for secondary analysis, because they underwent an emergency procedure. Compliance with the use of DAs was assessed in the included patients after implementation of DAs: 811 patients with gallstones and 898 patients with an inguinal hernia.

This flowchart of patient inclusion shows that 3423 patients were included to evaluate operation rates, patient compliance with decision aids was assessed in 1709 patients, and 155 patients responded to the questionnaire to assess satisfaction with final treatment and persistent pain
We contacted 322 patients to measure satisfaction with final treatment and persistent pain, five declined to participate, and 155 patients (48.1%) completed the questionnaire, 65 gallstone patients (response rate = 43.0%) and 90 hernia patients (response rate = 52.6%) (Fig. 1).
Operation rate
Operation rates for gallbladder removal and inguinal hernia repair in the intervention hospital substantially declined over the years 2014–2017 (Fig. 2). The average operation rate of gallbladder removal in the intervention hospital before the implementation of DAs was 72.0% (586/814) and after implementation 56.7% (460/811), a reduction of 15.3% (p < 0.001). For inguinal hernia, before implementation the average operation rate was 77.8% (700/900) and after implementation 64.6% (601/898), a reduction of 13.2% (p < 0.001).

Annual operation rates of the intervention hospital in 2014, 2015, 2016 and 2017
Decision aid compliance
In total, 512 out of 811 gallstones patients (63.1%) received a DA. Of these patients, 413 (80.7%) actually used the DA. For inguinal hernia, 528 out of 898 patients (58.8%) received a DA and 426 patients (80.7%) used the DA (Fig. 3).

Compliance with the use of decision aids is defined as use of a DA by patients, assessed by answers on all questions in step 3, 4 and 5 of the DA. Three groups of patients were identified: (1) patients who did not receive a DA (total patients minus patients who received a DA), (2) patients who received a DA but did not use it and (3) patients who received a DA and used it. The percentages of all three groups are presented in this chart
Satisfaction and persistent pain
One hundred and fifty-five patients responded to the questionnaire after a median follow-up of 11 months (inter-quartile range 9–13). In both conditions, the age of responders was significantly higher than in nonresponders (Tables 1, 2).
Of the 65 patients with gallstones who responded, 40 patients (61.5%) underwent a cholecystectomy and 25 patients (38.5%) were treated conservatively (Table 1). Of the responding inguinal hernia patients, 80% (n = 72) was operated and 20% of patients (n = 18) did not undergo surgery (Table 2). Satisfaction with final treatment was high in gallstone and inguinal hernia patients during follow-up; both patient groups scored a median 9.0 (range, respectively, 1–10 and 0–10). Of the patients with gallstones, 55 patients (84.6%) were pain-free and 80 patients (89.9%) with an inguinal hernia were pain-free. Pain-free rates and satisfaction with final treatment were higher in operated hernia patients compared to those nonoperated.
Discussion
The present study shows reduced elective operation rates and preservation of patient satisfaction after the implementation of DAs in patients with gallstones or an inguinal hernia. Our analysis shows a decrease of approximately 14% in operation rates for both conditions. About 60% of all new patients received the online DA, of whom 80% actually used it. Moreover, patients who used the DA scored high on satisfaction with final treatment and low on persistent pain, and pain-free rates were high.
Though the impact of DAs in general surgery has never been reported, in other types of surgery, evidence is evolving. Stacey et al. showed that DAs improve patients’ involvement in the decision-making process and reduce decisional conflict. A systematic review evaluated studies investigating the effect of DAs on SDM and surgical treatment decision in elective surgery [22]. DAs were evaluated in bariatric patients and patients with breast cancer, prostate cancer, lower back problems, menorrhagia, cystic fibrosis and asymptomatic abdominal aneurysm. Eight out of twelve studies demonstrated that patients with a DA more frequently opted for conservative or less-invasive treatment options compared to the control group [26,27,28,29,30,31,32,33]. Results were in line with another recent published review [34]. A recent systematic review, focusing on how to measure SDM in current practice and not on clinical effects, evaluated SDM in surgery and showed that SDM, despite the interest, was infrequent in surgery [19].
After we found decreased hospital rates after the intervention, we were interested how this finding is related to the nationwide averages in operation rates during the study period. For this comparison, the national DRG database was consulted (https://data.overheid.nl/data/dataset/open-dis-data, accessed November 2018) which showed a nationwide operation rate for gallbladder removal and hernia repair rates of approximately 70%. These national rates are 6–14% higher than the operation rates observed at our institution following the DA intervention.
This study is the first to show a decrease in operation rates in gallbladder removal and inguinal hernia repair after implementation of DAs and preservation of excellent patient satisfaction with final treatment. By the inclusion of an unselected patient population for the primary outcome measure, we were able to assess the impact of an online DA in a general, uncontrolled practice. However, the retrospective design also comes with several limitations. First, no data were available of patients who did not receive or use the DA, as well as no exact numbers for the reasons why patients did not receive or used the DA. Second, only a prepost analysis was performed and multivariable regression analyses could not be performed due to missing variables and small patients groups in secondary analysis. An institutional reduction in operation capacity, changes in referral patterns, collaboration with other hospitals during the study period are all potential factors influencing operation rates. However, none of these seem to apply to the intervention hospital. SDM was not measured in this study; however, many studies already showed the effectiveness of DAs to reduce decisional conflict and patient involvement in the decision-making process. Moreover, as we were not able to discriminate complicated and noncomplicated conditions (e.g., cholecystitis and non-reducible hernia) based on the DRG codes, the estimated operation rates may be an overestimation of the operation rate that should be affected by the DA, i.e., in patients with an uncomplicated condition. However, we excluded all patients with an emergency operation, so this overestimation will be small. The decrease in the operation rate in 2015 could be explained by the start of the project entitled Shared Decision initiated that year (https://www.bernhoven.nl/samenbeslissen).
Pain-free rates found in our study were far higher compared to previously published studies [35,36,37]. This could be explained by altered patient’s perceptions due to the preoperative DA. As a result of the DAs, patients are actively involved in the decision of treatment and are better informed about complications and persistent symptoms [20]. Potentially, patients experience persistent symptoms less or differently. To further investigate the effect of DAs on operation rates and patient satisfaction, a prospective study design is required, performed with validated questionnaires on several time points. Our study group has initiated a prospective study (Dutch Trial Register NTR7501) which needs to confirm present findings in a larger cohort of patients. The long-term results of this study will show whether or not an initial decision to refrain from surgery turns into definitive conservative treatment on the long term.
This study reports a high rate of patients’ compliance using the DA. However, DAs were only provided to approximately 60% of patients. There are several reasons why not all patients received a DA: some patients were not eligible for a DA, as watchful waiting or surgery was not an option for these patients, and patients were illiterate or physicians forgot to provide a DA. The latter should be avoided when DAs become standard care. Unfortunately, no data were available about exact prevalence of reasons. Reasons will be count in the initiated prospective study.
As the present study illustrates a potential operation reduction of 14% for both conditions, it is of economic interest to estimate the potential cost effectiveness of a nationwide implementation of DAs for the conditions of interest. Annually, in the Netherlands, 34,000 patients present with gallstone disease and 33,000 with an inguinal hernia; the annual operation rate is 73% and 72%, and direct surgical costs are 4000 and 2000 euro’s, respectively [38]. We excluded 20% of patients from this estimated cost reduction, due to complicated disease. Assuming a reduction of 12% (with inclusion of patients with an emergency operation) for both conditions in operation rates (even when only 60% of patients received a DA), the associated potential cost savings are up to €19.4 million annually. Only if proven cost-effective, then DAs are very likely to be affordable and need (inter) national implementation in daily surgical care.
In conclusion, the present analysis is the first to show reduced elective operation rates after the implementation of DAs in gallbladder removal and inguinal hernia repair. Compliance with the use of DAs is high, patients are satisfied with the final treatment, and DAs for patients with gallstones or an inguinal hernia potentially result in more pain-free patients.
References
Russo MW, Wei JT, Thiny MT et al (2004) Digestive and liver diseases statistics, 2004. Gastroenterology 126:1448–1453
Schumpelick V, Treutner KH, Arlt G (1994) Inguinal hernia repair in adults. Lancet (London, England) 344:375–379
Jatzko GR, Lisborg PH, Pertl AM et al (1995) Multivariate comparison of complications after laparoscopic cholecystectomy and open cholecystectomy. Ann Surg 221:381–386
Felix EL, Harbertson N, Vartanian S (1999) Laparoscopic hernioplasty: significant complications. Surg Endosc 13:328–331
Fitzgibbons RJ Jr, Camps J, Cornet DA et al (1995) Laparoscopic inguinal herniorrhaphy. Results of a multicenter trial. Ann Surg 221:3–13
Phillips EH, Arregui M, Carroll BJ et al (1995) Incidence of complications following laparoscopic hernioplasty. Surg Endosc 9:16–21
de Goede B, Wijsmuller AR, van Ramshorst GH et al (2018) Watchful waiting versus surgery of mildly symptomatic or asymptomatic inguinal hernia in men aged 50 years and older: a randomized controlled trial. Ann Surg 267:42–49
Vetrhus M, Soreide O, Eide GE et al (2004) Pain and quality of life in patients with symptomatic, non-complicated gallbladder stones: results of a randomized controlled trial. Scand J Gastroenterol 39:270–276
Oliver MN (2003) Watchful waiting is reasonable for gallstone symptoms. The Journal of family practice 52:18–20
McSherry CK, Ferstenberg H, Calhoun WF et al (1985) The natural history of diagnosed gallstone disease in symptomatic and asymptomatic patients. Ann Surg 202:59–63
Fitzgibbons RJ, Jonasson O, Gibbs J et al (2003) The development of a clinical trial to determine if watchful waiting is an acceptable alternative to routine herniorrhaphy for patients with minimal or no hernia symptoms. J Am Coll Surg 196:737–742
Jenkins JT, O’Dwyer PJ (2008) Inguinal hernias. BMJ: Bt Med J 336:269–272
Friedman GD (1993) Natural history of asymptomatic and symptomatic gallstones. Am J Surg 165:399–404
Halldestam I, Enell E-L, Kullman E et al (2004) Development of symptoms and complications in individuals with asymptomatic gallstones. BJS 91:734–738
Uldry E, Schafer M, Saadi A et al (2013) Patients’ preferences on information and involvement in decision making for gastrointestinal surgery. World J Surg 37:2162–2171. https://doi.org/10.1007/s00268-013-2084-8
Elwyn G, Frosch D, Thomson R et al (2012) Shared decision making: a model for clinical practice. J Gen Intern Med 27:1361–1367
Barratt A (2008) Evidence based medicine and shared decision making: the challenge of getting both evidence and preferences into health care. Patient Educ Couns 73:407–412
Ubbink DT, Hageman MG, Legemate DA (2015) Shared decision-making in surgery. Surg Technol Int 26:31–36
de Mik SML, Stubenrouch FE, Balm R et al (2018) Systematic review of shared decision-making in surgery. BJS 105:1721–1730
Stacey D, Legare F, Lewis K et al (2017) Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev 4:CD001431
Stiggelbout AM, Pieterse AH, De Haes JC (2015) Shared decision making: concepts, evidence, and practice. Patient Educ Couns 98:1172–1179
Knops AM, Legemate DA, Goossens A et al (2013) Decision aids for patients facing a surgical treatment decision: a systematic review and meta-analysis. Ann Surg 257:860–866
Vandenbroucke JP, von Elm E, Altman DG et al (2014) Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Int J Surg (London, England) 12:1500–1524
Jensen MP, Chen C, Brugger AM (2003) Interpretation of visual analog scale ratings and change scores: a reanalysis of two clinical trials of postoperative pain. J Pain: Off J Am Pain Soc 4:407–414
de Reuver PR, van Dijk AH, Wennmacker SZ et al (2016) A randomized controlled trial to compare a restrictive strategy to usual care for the effectiveness of cholecystectomy in patients with symptomatic gallstones (SECURE trial protocol). BMC Surg 16:46
Arterburn D, Wellman R, Westbrook E et al (2012) Introducing decision aids at Group Health was linked to sharply lower hip and knee surgery rates and costs. Health Aff (Millwood) 31:2094–2104
Deyo RA, Cherkin DC, Weinstein J et al (2000) Involving patients in clinical decisions: impact of an interactive video program on use of back surgery. Med Care 38:959–969
Kennedy AD, Sculpher MJ, Coulter A et al (2002) Effects of decision aids for menorrhagia on treatment choices, health outcomes, and costs: a randomized controlled trial. JAMA 288:2701–2708
Molenaar S, Sprangers MA, Rutgers EJ et al (2001) Decision support for patients with early-stage breast cancer: effects of an interactive breast cancer CDROM on treatment decision, satisfaction, and quality of life. J Clin Oncol 19:1676–1687
Auvinen A, Hakama M, Ala-Opas M et al (2004) A randomized trial of choice of treatment in prostate cancer: the effect of intervention on the treatment chosen. BJU Int 93:52–56 discussion 56
Whelan T, Levine M, Willan A et al (2004) Effect of a decision aid on knowledge and treatment decision making for breast cancer surgery: a randomized trial. JAMA 292:435–441
Vandemheen KL, O’Connor A, Bell SC et al (2009) Randomized trial of a decision aid for patients with cystic fibrosis considering lung transplantation. Am J Respir Crit Care Med 180:761–768
Vodermaier A, Caspari C, Koehm J et al (2009) Contextual factors in shared decision making: a randomised controlled trial in women with a strong suspicion of breast cancer. Br J Cancer 100:590–597
Boss EF, Mehta N, Nagarajan N et al (2016) Shared decision-making and choice for elective surgical care: A systematic review. Otolaryngol Head Neck Surg 154:405–420
Lamberts MP, Lugtenberg M, Rovers MM et al (2013) Persistent and de novo symptoms after cholecystectomy: a systematic review of cholecystectomy effectiveness. Surg Endosc 27:709–718
Wennmacker S, Lamberts M, Gerritsen J et al (2017) Consistency of patient-reported outcomes after cholecystectomy and their implications on current surgical practice: a prospective multicenter cohort study. Surg Endosc 31:215–224
Vetrhus M, Berhane T, Soreide O et al (2005) Pain persists in many patients five years after removal of the gallbladder: observations from two randomized controlled trials of symptomatic, noncomplicated gallstone disease and acute cholecystitis. J Gastrointest Surg 9:826–831
Dutch Health Care Authority (Nederlandse Zorgautoriteit) (2017) DRG Database (Open DIS data)
Author information
Authors and Affiliations
Contributions
Conception and design, acquisition of data, analysis and interpretation, and drafting the article were done by CL. Interpretation of data and revising article were done by BW, MK, MM, BT. Conception and design, interpretation of data, and revising article were done by PR. All authors approved the final version. All authors agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Conflict of interest
All authors have no conflicts of interest or financial ties to disclose.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Ethical statement
The study was approved by the appropriate institution and/or national research ethics committee (registration number 2017-3973).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix: Decision aids
Appendix: Decision aids
The online DAs were developed by patients and physicians according to the International Patient Decision Aids Standards (IPDAS) and comprise five steps (http://ipdas.ohri.ca/). The first step informs the patient about the diagnosis and the two treatment options: surgery and watchful waiting. Both laparoscopic surgery and open surgery are explained; these surgical procedures were not compared to each other. Step two informs about the benefits, harms, scientific uncertainties and probabilities of outcome, and this is summarized in a table. In step three, the most important information is again brought under attention in the form of a knowledge questionnaire. In step four, a value clarification exercise is carried out, asking the patient to consider which benefits and risks matter most to them. In step five, the patient is asked to reflect on their response and to point out their preferred treatment (https://www.decisionaid.info).
Experience showed that introduction of DAs only is not enough and attention must also be paid to creating a mind shift among the entire staff and patients, so the introduction of DAs was accompanied by an implementation strategy, a training SDM for the involved physicians. The implementation of DAs (introduction of DAs and training SDM) was part of the project Shared Decision (“Samen Beslissen”), which started in 2015 in collaboration with the Dutch Patient Federation (https://www.bernhoven.nl/samenbeslissen).
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Latenstein, C.S.S., van Wely, B.J., Klerkx, M. et al. Reduced Elective Operation Rates and High Patient Satisfaction After the Implementation of Decision Aids in Patients with Gallstones or an Inguinal Hernia. World J Surg 43, 2149–2156 (2019). https://doi.org/10.1007/s00268-019-05007-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-019-05007-w