
Abstract
Background
Breast carcinoma presented with nipple discharge is a rare condition. There is theoretical concern about preserving nipple in these patients since the risk of nipple–areolar complex involvement may be greater, but not many studies in the literature have addressed on this issue. The aim of the current study was to determine the incidence and outcome of nipple preservation in breast cancer associated with nipple discharge.
Methods
Medical records of patients who were diagnosed to have breast carcinoma and presented with nipple discharge from May 2009 to October 2014 were retrospectively reviewed.
Results
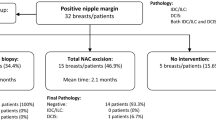
Sixty patients presented with nipple discharge were diagnosed with breast cancer, which represent 3.8 % of all patients who underwent breast cancer surgery in our unit during the study period. Forty-six patients (76.7 %) had nipple discharge as their only symptom, while the rest also presented with breast mass clinically or radiologically. All patients had mammogram and ultrasound performed, and 53.3 and 63.3 % respectively showed suspicious findings. Forty-one out of 46 (89.1 %) nipple discharge cytology were inadequate or benign. Thirty-two microdochectomy were performed. Routine frozen section was utilized intra-operatively to ensure clear margins. The most common histology was ductal carcinoma in situ (DCIS) (n = 29, 48.3 %), followed by DCIS with invasive ductal carcinoma (n = 23, 38.3 %). Regarding treatment, 26 patients (43.3 %) had nipple preserved, including 21 breast conservative surgery and five nipple-sparing mastectomies. Overall, no local or systemic recurrence was observed at a median follow-up of 27 months. Ten out of 34 (29.4 %) mastectomy specimens showed NAC involvement on pathology. By comparing patients with NAC preserved to patients with NAC removed, no significant preoperative predictors were identified.
Conclusion
Breast carcinoma patients who present with nipple discharge usually have early-stage cancer. Presence of nipple discharge is not equivalent to NAC involvement. Nipple preservation can be oncologically safe if negative margins are ascertained.
Similar content being viewed by others


References
Seltzer MH (2004) Breast complaints, biopsies, and cancer correlated with age in 10,000 consecutive new surgical referrals. Breast J 10(2):111–117
Galvin R, Joyce D, Downey E, Boland F, Fahey T, Hill AK (2014) Development and validation of a clinical prediction rule to identify suspected breast cancer: a prospective cohort study. BMC Cancer 14:743
Lau S, Küchenmeister I, Stachs A, Gerber B, Krause A, Reimer T (2005) Pathologic nipple discharge: surgery is imperative in postmenopausal women. Ann Surg Oncol 12(7):546–551
Leis JHP (1989) Management of nipple discharge. World J Surg 13(6):736–742
Carpenter A, Adamson A, Royle GT (1989) A prospective study of nipple discharge. Br J Clin Pract Suppl 68:54–57
Wertheim U, Ozzello L (1980) Neoplastic involvement of nipple and skin flap in carcinoma of the breast. Am J Surg Pathol 4(6):543–549
Kissin M, Kark A (1987) Nipple preservation during mastectomy. Br J Surg 74(1):58–61
Laronga C, Kemp B, Johnston D (1999) The incidence of occult nipple–areola complex involvement in breast cancer patients receiving a skin-sparing mastectomy. Ann Surg Oncol 6(6):609–613
Lambert PA, Kolm P, Perry RR (2000) Parameters that predict nipple involvement in breast cancer. J Am Coll Surg 191(4):354–359
Simmons RM, Brennan M, Christos P (2002) Analysis of nipple/areolar involvement with mastectomy: can the areola be preserved? Ann Surg Oncol 9(2):165–168
Tancredi A, Ciuffreda L, Petito L, Natale F, Murgo R (2013) Nipple–areola-complex sparing mastectomy: five years of experience in a single centre. Updates Surg 65(4):289–294
Rocco N, Catanuto G, Nava MB (2015) What is the evidence behind conservative mastectomies? Gland Surg 4(6):506–518
Wei CH, Scott AM, Price AN, Miller HC, Klassen AF, Jhanwar SM et al (2016) Psychosocial and sexual well-being following nipple-sparing mastectomy and reconstruction. Breast J 22(1):10–17
Murthy V, Chamberlain RS (2013) Defining a place for nipple sparing mastectomy in modern breast care: an evidence based review. Breast J 19(6):571–581
Cabioglu N, Krishnamurthy S, Kuerer HM, Hunt KK, Singletary SE, Meric-Bernstam F et al (2004) Feasibility of breast-conserving surgery for patients with breast carcinoma associated with nipple discharge. Cancer 101(3):508–517
Cheung P, Hung WK, Cheung C, Chan A, Wong TT, Li L et al (2012) Early data from the first population-wide breast cancer-specific registry in Hong Kong. World J Surg 36(4):723–729
Eisenberg RE, Chan JS, Swistel AJ, Hoda SA (2014) Pathological evaluation of nipple-sparing mastectomies with emphasis on occult nipple involvement: the Weill–Cornell experience with 325 cases. Breast J 20(1):15–21
Kryvenko ON, Yoon JY, Chitale DA, Lee MW (2013) Prevalence of terminal duct lobular units and frequency of neoplastic involvement of the nipple in mastectomy. Arch Pathol Lab Med 137(7):955–960
Mallon P, Feron JG, Couturaud B, Fitoussi A, Lemasurier P, Guihard T et al (2013) The role of nipple-sparing mastectomy in breast cancer: a comprehensive review of the literature. Plast Reconstr Surg 131(5):969–984
Zhang H, Li Y, Moran MS, Haffty BG, Yang Q (2015) Predictive factors of nipple involvement in breast cancer: a systematic review and meta-analysis. Breast Cancer Res Treat 151(2):239–249
Karamchandani DM, Chetlen AL, Riley MP, Schetter S, Hollenbeak CS, Mack J (2015) Pathologic–radiologic correlation in evaluation of retroareolar margin in nipple-sparing mastectomy. Virchows Arch 466(3):279–287
D'Alonzo M, Martincich L, Biglia N, Pisacane A, Maggiorotto F, Rosa GD et al (2012) Clinical and radiological predictors of nipple–areola complex involvement in breast cancer patients. Eur J Cancer 48(15):2311–2318
Moon JY, Chang YW, Lee EH, Seo DY (2013) Malignant invasion of the nipple–areolar complex of the breast: usefulness of breast MRI. Am J Roentgenol (AJR) 201(2):448–455
Van Gelder L, Bisschops RH, Menke-Pluymers MB, Westenend PJ, Plaisier PW (2015) Magnetic resonance imaging in patients with unilateral bloody nipple discharge; useful when conventional diagnostics are negative? World J Surg 39(1):184–186
Saricaa O, Ozturkb E, Demirkurekc HC, Uluca F (2013) Comparison of ductoscopy, galactography, and imaging modalities for the evaluation of intraductal lesions: a critical review. Breast Care 8(5):348–354
Ohlinger R, Stomps A, Paepke S, Blohmer JU, Grunwald S, Hahndorf W et al (2014) Ductoscopic detection of intraductal lesions in cases of pathologic nipple discharge in comparison with standard diagnostics: the German multicenter study. Oncol Res Treat 37(11):628–632
Kneubil MC, Lohsiriwat V, Curigliano G, Brollo J, Botteri E, Rotmensz N et al (2012) Risk of locoregional recurrence in patients with false-negative frozen section or close margins of retroareolar specimen in nipple-sparing mastectomy. Ann Surg Oncol 19(13):4117–4123
Morales-Piato JR, Aguiar FN, Mota BS, Ricci MD, Dória MT, Alves-Jales RD et al (2015) Improved frozen section examination of the retroareolar margin for prediction of nipple involvement in breast cancer. Eur J Surg Oncol 41(8):986–990
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chang, R.Y.K., Cheung, P.S.Y. Nipple Preservation in Breast Cancer Associated with Nipple Discharge. World J Surg 41, 176–183 (2017). https://doi.org/10.1007/s00268-016-3679-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-016-3679-7