
Abstract
Background
Whether total extraperitoneal inguinal hernia repair (TEP) is associated with worse outcomes compared to transabdominal preperitoneal inguinal hernia repair (TAPP) for the treatment of recurrent inguinal hernia continues to be a matter of debate. The objective of this large cohort study is to compare complications, conversion rates and postoperative length of hospital stay between patients undergoing TEP or TAPP for unilateral recurrent inguinal hernia repair.
Method
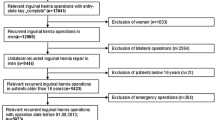
Based on prospective data of the Swiss Association of Laparoscopic and Thoracoscopic Surgery, all patients who underwent elective TEP or TAPP for unilateral recurrent inguinal hernia between 1995 and 2006 were included. The following outcomes were compared: conversion rates, intraoperative complications, surgical postoperative complications and duration of operation.
Results
Data on 1309 patients undergoing TEP (n = 1022) and TAPP (n = 287) for recurrent inguinal hernia were prospectively collected. Average age, BMI and ASA score were similar in both groups. Patients undergoing TEP had a significantly increased rate of intraoperative complications (TEP 6.3 % vs. TAPP 2.8 %, p = 0.0225). Duration of operation was longer for patients undergoing TEP (TEP 80.3 vs. TAPP 73.0 min, p < 0.0023) while postoperative length of hospital stay was longer for patients undergoing TAPP (TEP 2.6 vs. TAPP 3.1 day, p = 0.0145). Surgical postoperative complications (TEP 3.52 % vs. TAPP 2.09 %, p = 0.2239), general postoperative complications (TEP 1.47 % vs. TAPP 0.7 %, p = 0.3081) and conversion rates (TEP 2.15 % vs. TAPP 1.39 %, p = 0.4155) were not significantly different.
Conclusion
This study is the first population-based analysis comparing outcomes of patients with recurrent inguinal hernia undergoing TEP versus TAPP in a prospective cohort of over 1300 patients. Intraoperative complications were significantly higher in patients undergoing TEP. The TEP technique was associated with longer operating times, but a shorter postoperative length of hospital stay. Nonetheless, the absolute outcome differences are small and thus, on a population-based level, both techniques appear to be safe and effective for patients undergoing endoscopic repair for unilateral recurrent inguinal hernia.
Similar content being viewed by others

References
Rutkow IM (2003) Demographic and socioeconomic aspects of hernia repair in the United States in 2003. Surg Clin North Am 83:1045–1051
Haapaniemi S, Gunnarsson U, Nordin P et al (2001) Reoperation after recurrent groin hernia repair. Ann Surg 234:122–126
Gass M, Banz VM, Rosella L et al (2012) TAPP or TEP? Population-based analysis of prospective data on 4552 patients undergoing endoscopic inguinal hernia repair. World J Surg 36:2782–2786
Zendejas B, Onkendi EO, Brahmbhatt RD et al (2011) Long-term outcomes of laparoscopic totally extraperitoneal inguinal hernia repairs performed by supervised surgical trainees. Am J Surg 201(379–383):83–84
Wright D, O’Dwyer PJ (1998) The learning curve for laparoscopic hernia repair. Semin Laparosc Surg 5:227–232
Lal P, Kajla RK, Chander J et al (2004) Laparoscopic total extraperitoneal (TEP) inguinal hernia repair: overcoming the learning curve. Surg Endosc 18:642–645
Gass M, Rosella L, Banz V et al (2012) Bilateral total extraperitoneal inguinal hernia repair (TEP) has outcomes similar to those for unilateral TEP: population-based analysis of prospective data of 6505 patients. Surg Endosc 26:1364–1368
Tantia O, Jain M, Khanna S et al (2009) Laparoscopic repair of recurrent groin hernia: results of a prospective study. Surg Endosc 23:734–738
Pisanu A, Podda M, Saba A et al (2015) Meta-analysis and review of prospective randomized trials comparing laparoscopic and Lichtenstein techniques in recurrent inguinal hernia repair. Hernia 19:355–366
Karthikesalingam A, Markar SR, Holt PJ et al (2010) Meta-analysis of randomized controlled trials comparing laparoscopic with open mesh repair of recurrent inguinal hernia. Br J Surg 97:4–11
Shah NR, Mikami DJ, Cook C et al (2011) A comparison of outcomes between open and laparoscopic surgical repair of recurrent inguinal hernias. Surg Endosc 25:2330–2337
Guller U, Rosella L, Karanicolas PJ et al (2010) Population-based trend analysis of 2813 patients undergoing laparoscopic sigmoid resection. Br J Surg 97:79–85
Brugger L, Rosella L, Candinas D et al (2011) Improving outcomes after laparoscopic appendectomy: a population-based, 12-year trend analysis of 7446 patients. Ann Surg 253:309–313
Acknowledgments
The authors thank Dr. Laura Rosella and Prof. Dr. Ueli Güller for carefully reading the manuscript and making many valuable suggestions. This study was supported by grants from Johnson & Johnson and Covidien.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Drs. Markus Gass, Andreas Scheiwiller, Martin Sykora and Jürg Metzger have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Gass, M., Scheiwiller, A., Sykora, M. et al. TAPP or TEP for Recurrent Inguinal Hernia? Population-Based Analysis of Prospective Data on 1309 Patients Undergoing Endoscopic Repair for Recurrent Inguinal Hernia. World J Surg 40, 2348–2352 (2016). https://doi.org/10.1007/s00268-016-3545-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-016-3545-7