
Abstract
Introduction
The purpose of this article was to review the research considering fast-track concepts in upper abdominal and thoracoabdominal surgery.
Methods
A search for clinical studies evaluating the fast-track concept after open major upper abdominal or thoracoabdominal surgery was performed. Reference lists of identified articles were searched. Trials—written in English—that compared a concept and traditional care were evaluated with regard to their internal validity. Level of evidence was defined and each outcome was evaluated.
Results
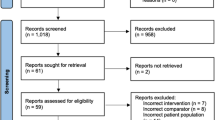
In total, 15 articles were found, separated into gastric (n = 2), pancreatic (n = 5), hepatic (n = 2), esophageal (n = 3), and aortic surgery (n = 3). Three were randomized, controlled trials. The different trials represented various concepts of fast-track surgery, but the majority included specific programs for analgesics, avoidance of drainage tubes, early start of oral nutrition, and early and active mobilization. There is moderate evidence that fast-track concepts result in shorter hospital stay. There is low evidence that fast-track concepts shorten need of ventilation, decrease the need of care at the intensive care unit, decrease postoperative pain, and reduce total hospital costs. The concepts seem to have similar rates of surgical complications, readmission rate, and mortality rates as conventional care. No specific adverse events were reported.
Conclusions
Although the methodological quality of the articles reviewed was low and the trials heterogeneous, all trials concluded that the introduction of fast-track concepts were safe and feasible, achieved shorter hospital stays, and reduced costs. Future randomized, controlled trials are needed to further evaluate the effect of these concepts.

Similar content being viewed by others


References
Kehlet H, Dahl JB (1993) The value of “multimodal” or “balanced analgesia” in postoperative pain treatment. Anesth Analg 77(5):1048–1056
Kehlet H, Wilmore DW (2008) Evidence-based surgical care and the evolution of fast-track surgery. Ann Surg 248(2):189–198
Basse L, Raskov HH, Hjort Jakobsen D et al (2002) Accelerated postoperative recovery programme after colonic resection improves physical performance, pulmonary function and body composition. Br J Surg 89(4):446–453
Hammer J, Harling H, Wille-Jørgensen P (2008) Implementation of the scientific evidence into daily practice—example from fast-track colonic cancer surgery. Colorectal Dis 10(6):593–598
Wichmann MW, Eben R, Angele MK et al (2007) Fast-track rehabilitation in elective colorectal surgery patients: a prospective clinical and immunological single-centre study. ANZ J Surg 77(7):502–507
Wind J, Polle SW, Fung Kon Jin PH et al (2006) Laparoscopy and/or Fast Track multimodal management versus standard care (LAFA) study group; enhanced recovery after surgery (ERAS) group. Systematic review of enhanced recovery programmes in colonic surgery. Br J Surg 93(7):800–809
van Tulder M, Furlan A, Bombardier C, Bouter L (2003) Updated method guidelines for systematic reviews in the Cochrane collaboration back review group. Spine 28:1290–1299
Wang D, Kong Y, Zhong B, Zhou X, Zhou YJ (2010) Fast-track surgery improves postoperative recovery in patients with gastric cancer: a randomized comparison with conventional postoperative care. Gastrointest Surg 14(4):620–627
Liu XX, Jiang ZW, Wang ZM, Li JS (2010) Multimodal optimization of surgical care shows beneficial outcome in gastrectomy surgery. JPEN J Parenter Enteral Nutr 34(3):313–321
Balzano G, Zerbi A, Braga M et al (2008) Fast-track recovery programme after pancreatico-duodenectomy reduces delayed gastric emptying. Br J Surg 95(11):1387–1393
Kennedy EP, Rosato EL, Sauter PK et al (2007) Initiation of a critical pathway for pancreaticoduodenectomy at an academic institution–the first step in multidisciplinary team building. J Am Coll Surg 204(5):917–923
Porter GA, Pisters PW, Mansyur C et al (2000) Cost and utilization impact of a clinical pathway for patients undergoing pancreaticoduodenectomy. Ann Surg Oncol 7(7):484–489
Berberat PO, Ingold H, Gulbinas A et al (2007) Fast track—different implications in pancreatic surgery. J Gastrointest Surg 11(7):880–887
di Sebastiano P, Festa L, De Bonis A et al (2011) A modified fast-track program for pancreatic surgery: a prospective single-center experience. Langenbecks Arch Surg 396(3):345–351
van Dam RM, Hendry PO, Coolsen MM et al (2008) Enhanced recovery after surgery (ERAS) group. Initial experience with a multimodal enhanced recovery programme in patients undergoing liver resection. Br J Surg 95(8):969–975
MacKay G, O’Dwyer PJ (2008) Early discharge following liver resection for colorectal metastases. Scott Med J 53(2):22–24
Muehling B, Schelzig H, Steffen P et al (2009) A prospective randomized trial comparing traditional and fast-track patient care in elective open infrarenal aneurysm repair. World J Surg 33(3):577–585
Murphy MA, Richards T, Atkinson C et al (2007) Fast track open aortic surgery: reduced post operative stay with a goal directed pathway. Eur J Vasc Endovasc Surg 34(3):274–278
Brustia P, Renghi A, Fassiola A et al (2007) Fast-track approach in abdominal aortic surgery: left subcostal incision with blended anesthesia. Interact Cardiovasc Thorac Surg 6(1):60–64
Brodner G, Pogatzki E, Van Aken H et al (1998) A multimodal approach to control postoperative pathophysiology and rehabilitation in patients undergoing abdominothoracic esophagectomy. Anesth Analg 86(2):228–234
Cerfolio RJ, Bryant AS, Bass CS et al (2004) Fast tracking after Ivor Lewis esophagogastrectomy. Chest 126(4):1187–1194
Neal JM, Wilcox RT, Allen HW, Low DE (2003) Near-total esophagectomy: the influence of standardized multimodal management and intraoperative fluid restriction. Reg Anesth Pain Med 28(4):328–334
Lemmens L, van Zelm R, Borel Rinkes I et al (2009) Clinical and organizational content of clinical pathways for digestive surgery: a systematic review. Dig Surg 26(2):91–99
Diks J, van Hoorn DE, Nijveldt RJ et al (2005) Preoperative fasting: an outdated concept? JPEN J Parenter Enteral Nutr 29(4):298–304
Harper CM, Lyles YM (1988) Physiology and complications of bed rest. J Am Geriatr Soc 36(11):1047–1054
Low DE, Kunz S, Schembre D, Otero H et al (2007) Esophagectomy—it’s not just about mortality anymore: standardized perioperative clinical pathways improve outcomes in patients with esophageal cancer. J Gastrointest Surg 11(11):1395–1402
Conflicts of interest
The work with this article was carried out without any grant support. There are no potential and real conflicts of interest concerning the content in this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fagevik Olsén, M., Wennberg, E. Fast-Track Concepts in Major Open Upper Abdominal and Thoracoabdominal Surgery: A Review. World J Surg 35, 2586–2593 (2011). https://doi.org/10.1007/s00268-011-1241-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-011-1241-1