
Abstract
Background
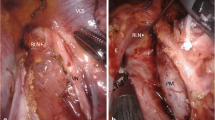
Patients who undergo surgery to the esophagus and lungs are in jeopardy of recurrent laryngeal nerve (RLN) damage during the procedure. This study was designed to investigate the feasibility of intraoperative monitoring of the RLN for single-lung ventilation esophagus and lung surgery.
Methods
Twelve consecutive patients booked for esophagus or lung surgery were included in this prospective, observational study. Six patients underwent transthoracic esophagectomy for carcinoma of the esophagogastric junction or lower esophagus, five had a lobectomy, and one underwent a pneumonectomy for lung carcinoma. Intraoperative, noninvasive RLN identification and monitoring was performed unilaterally (n = 8) or bilaterally (n = 4) using a handheld stimulator and a laryngeal surface electrode. The correct functioning of the nerve monitoring system was tested directly at the vagus nerve. Diagnosis of postoperative RLN paralysis was performed using indirect laryngoscopy.
Results
During the surgical procedures, we monitored a nerve signal in all 12 patients. In one patient with lower esophagus carcinoma, a nerve signal could be detected only on one side. Postoperative indirect laryngoscopy showed normal vocal cord movement in all patients.
Conclusions
Intraoperative RLN identification and monitoring during single-lung ventilation surgery is technically feasible, easy, and reliable. The introduction of standardized RLN monitoring during this type of surgery may reduce the incidence of permanent RLN paralysis.

Similar content being viewed by others


References
Sittel C, Stennert E, Thumfart WF et al (2001) Prognostic value of laryngeal electromyography in vocal fold paralysis. Arch Otolaryngol Head Neck Surg 127:155–160
Gockel I, Kneist W, Keilmann A et al (2005) Recurrent laryngeal nerve paralysis (RLNP) following esophagectomy for carcinoma. Eur J Surg Oncol 31:277–281
Johnson PR, Kanegoanker GS, Bates T (1994) Indirect laryngoscopic evaluation of vocal cord function in patients undergoing transhiatal esophagectomy. J Am Coll Surg 178:605–608
Filaire M, Mom T, Laurent S et al (2001) Vocal cord dysfunction after left lung resection for cancer. Eur J Cardiothorac Surg 20:705–711
Merati AL, Shemirani N, Smith TL et al (2006) Changing trends in the nature of vocal fold motion impairment. Am J Otolaryngol 27:106–108
Hemmerling TM, Schurr C, Dern S et al (2000) Intraoperative electromyographic recurrent laryngeal nerve identification as a routine measure. Chirurg 71:545–550
Riddell VH (1956) Injury to recurrent laryngeal nerves during thyroidectomy. A comparison between the results of identification, non-identification in 1022 nerves exposed to risk. Lancet 29:638–664
Dralle H, Sekulla C, Haerting J et al (2004) Risk factors of paralysis and functional outcome after recurrent laryngeal nerve monitoring in thyroid surgery. Surgery 136:1310–1322
Hermann M, Hellebart C, Freissmuth M (2004) Neuromonitoring in thyroid surgery: prospective evaluation of intraoperative electrophysiological responses for the prediction of recurrent laryngeal nerve injury. Ann Surg 240:9–17
Myssiorek D (2004) Recurrent laryngeal nerve paralysis: anatomy and etiology. Otolaryngol Clin N Am 37:25–44
Schulte KM, Roher HD (2001) Complications in the surgery of benign thyroid disease. Acta Chir Austriaca 33:164–172
Fang WT, Chen WH, Chen Y et al (2007) Selective three-field lymphadenectomy for thoracic esophageal squamous carcinoma. Dis Esophagus 20:206–211
Disclosures
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gelpke, H., Grieder, F., Decurtins, M. et al. Recurrent Laryngeal Nerve Monitoring During Esophagectomy and Mediastinal Lymph Node Dissection. World J Surg 34, 2379–2382 (2010). https://doi.org/10.1007/s00268-010-0692-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-010-0692-0