
Abstract
Background
A proportion of patients with chronic anal fissure have persistent symptoms and pathology despite optimum conservative therapies. Lateral anal sphincterotomy, the standard surgical treatment, is associated with functional compromise in a minority of patients. Sphincter-sparing anoplasty has been advocated as an alternative procedure for those with “low pressure” sphincters. The aim of this study was to determine the efficacy of simple cutaneous advancement flap anoplasty (SCAFA) when applied to consecutive patients with chronic anal fissure irrespective of anal tone and the patient’s gender.
Method
This was a prospective outcome study of 51 consecutive patients treated with SCAFA over a 6.5-year period.
Results
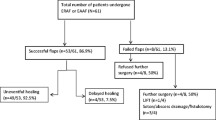
Surgery was well tolerated. There were three (5.9%) early flap dehiscences, all of which were treated with repeat SCAFA, and one of those three patients remained symptomatic at 2 months. All fissures healed in the short term. Three other patients subsequently developed fissures at sites remote from the original pathology. Continence was unaffected by the procedure.
Conclusions
Simple cutaneous advancement flap anoplasty should be considered as a first-line surgical treatment of chronic anal fissure, irrespective of patient gender and anal tone.


Similar content being viewed by others


References
Loder PB, Kamm MA, Nicholls RJ et al (1994) “Reversible chemical sphincterotomy” by local application of glyceryl trinitrate. Br J Surg 81:1386–1389
Schouten WR, Briel JW, Auwerda JJ et al (1996) Ischaemic nature of anal fissure. Br J Surg 83:63–65
Jonas M, Scholefield JH (2001) Anal fissure. Gastroenterol Clin North Am 30:1667–1681
Notaras MJ (1969) Lateral subcutaneous sphincterotomy for anal fissure—a new technique. Proc R Soc Med 62:713
Notaras MJ (1971) The treatment of anal fissure by lateral subcutaneous sphincterotomy—a technique and results. Br J Surg 58:96–100
Nyam DC, Pemberton JH (1999) Long-term results of lateral internal sphincterotomy in patients with chronic anal fissure with particular reference to incidence of fecal incontinence. Dis Colon Rectum 10:1306–1310
Lindsey I, Jones OM, Cunningham C et al (2004) Chronic anal fissure. Br J Surg 91:270–279
Ortiz H, Marzo J, Armendariz P et al (2005) Quality of life assessment in patients with chronic anal fissure after lateral internal sphincterotomy. Br J Surg 92:881–885
Casillas S, Hull TL, Zutshi M (2005) Incontinence after a lateral internal sphincterotomy: are we underestimating it? Dis Colon Rectum 16:1193–1199
Lunniss PJ, Gladman MA, Hetzer FH et al (2004) Risk factors in acquired faecal incontinence. J R Soc Med 97:111–116
Engel AF, Eijsbouts QAJ, Balk AG (2002) Fissurectomy and isosorbide dinitrate for chronic fissure in ano not responding to conservative treatment. Br J Surg 89:79–83
Scholz Th, Hetzer FH, Dindo D et al (2007) Long-term follow-up after combined fissurectomy and Botox injection for chronic anal fissures. Int J Colorect Dis 22:1077–1081
Habr-Gama A, Sobrado CW, de Araujo SE et al (2005) Surgical treatment of anal stenosis: assessment of 77 anoplasties. Clinics 60:17–20
Gonzalez AR, de Oliveira O, Verzaro R Jr et al (1995) Anoplasty for stenosis and other anorectal defects. Am Surg 61:526–529
Owen HA, Edwards DP, Khosraviani K et al (2006) The house advancement anoplasty for treatment of anal disorders. J R Army Med Corps 152:87–88
Samson RB, Stewart WRC (1970) Sliding skin grafts in the treatment of anal fissures. Dis Colon Rectum 13:372–375
Kenefick NJ, Gee AJ, Durdey P (2002) Treatment of resistant anal fissure with advancement anoplasty. Colorect Dis 4:463–466
Nyam DC, Wilson RG, Steward KJ et al (1995) Island advancement flaps in the management of anal fissures. Br J Surg 82:326–328
Singh M, Sharma A, Gardiner A et al (2005) Early results of a rotational flap to treat chronic anal fissures. Int J Colorect Dis 20:339–342
Leong AFPK, Seow-Choen F (1995) LAS compared with anal advancement flap for chronic anal fissure. Dis Colon Rectum 38:69–71
Porrett T, Knowles CH, Lunniss PJ (2003) Creation of a treatment protocol for nurse-led management of anal fissure. Colorect Dis 5:63–72
Nelson R (2006) Non surgical therapy for anal fissure. Cochrane Database Syst Rev 18:CD003431
Minguez M, Herreros B, Espi A et al (2002) Long-term follow-up (42 months) of chronic anal fissure after healing with botulinum toxin. Gastroenterology 123:112–117
Arroyo A, Pérez F, Serrano P et al (2005) Surgical versus chemical (botulinum toxin) sphincterotomy for chronic anal fissure: long-term results of a prospective randomized clinical and manometric study. Am J Surg 189:429–434
Nelson R (2005) Operative procedures for fissure in ano. Cochrane Database Syst Rev 18:CD002199
Brown CJ, Dubreuil D, Santoro L et al (2007) Lateral internal sphincterotomy is superior to topical nitroglycerin for healing chronic anal fissure and does not compromise long term fecal continence: six-year follow up of a multicenter, randomized, controlled trial. Dis Colon Rectum 50:442–448
Carapeti E, Kamm MA, McDonald PJ et al (1998) Double-blind randomized controlled trial of effect of metronidazole on pain after day case haemorrhoidectomy. Lancet 351:169–172
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Giordano, P., Gravante, G., Grondona, P. et al. Simple Cutaneous Advancement Flap Anoplasty for Resistant Chronic Anal Fissure: A Prospective Study. World J Surg 33, 1058–1063 (2009). https://doi.org/10.1007/s00268-009-9937-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-009-9937-1