
Abstract
Background
Admission hypothermia (core temperature ≤ 35°C) is an independent risk factor for mortality after trauma. The predictive value of perioperative core temperatures during acute trauma surgery, however, although widely employed as a criterion for initiating damage control, is unknown. We hypothesized that for trauma patients undergoing laparotomy or thoracotomy, early postoperative hypothermia is a predictor of mortality.
Methods
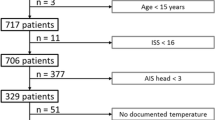
After institutional review board (IRB) approval, all critically ill trauma patients undergoing cavitary surgery (laparotomy or thoracotomy) at a level 1 trauma center from 01/1998 to 07/2006 were identified from the trauma registry. Immediate postoperative core temperature (Tc) was used to classify patients as hypothermic (Tc ≤ 35°C) or normothermic (Tc > 35°C). The profoundly hypothermic subgroup of patients with a Tc < 33°C was also analyzed.
Results
During the study period, 2,489 patients required cavitary surgery, 1,252 of whom (50%) were admitted to the intensive care unit (ICU). On arrival in the ICU 15% of the patients had a Tc ≤ 35°C and were more likely to be ≥ 55 years old (12% versus 7%; p = 0.04); in addition, they were hypotensive on admission (25% versus 13%; p < 0.001), had a lower admission Glasgow Coma Score (GCS; 11 ± 5 versus 14 ± 3; p < 0.001), a higher Injury Severity Score (ISS; 29 ± 15 versus 22 ± 12; p < 0.001), higher head and chest Abbreviated Injury Scale (AIS), and greater intraoperative blood loss (2.6 ± 2.4 l versus 1.7 ± 1.8 l; p < 0.001). When compared to patients who were normothermic at the end of their operation, hypothermic patients had a significantly higher mortality (35% versus 8%; p < 0.001). With decreasing Tc, there was a stepwise increase in mortality. Compared to patients with a Tc > 35°C, the relative risk of death for patients with a Tc between 35°C and 33°C was 4.0, and that for patients with a Tc ≤ 33°C it was 7.1. After adjusting for multiple differences between groups, postoperative hypothermia remained an independent predictor of mortality (adjusted odds ratio [OR] 3.2; 95% confidence interval [CI] 1.9–5.3; p < 0.001).
Conclusions
Postoperative hypothermia is common in critically injured patients requiring cavitary surgery and is an independent predictor of mortality. The impact of measures to maintain or restore normothermia in the operating room warrants further investigation.


Similar content being viewed by others


References
Wang HE, Callaway CW, Peitzman AB et al (2005) Admission hypothermia and outcome after major trauma. Crit Care Med 33:1296–1301
Shafi S, Elliott AC, Gentilello L (2005) Is hypothermia simply a marker of shock and injury severity or an independent risk factor for mortality in trauma patients? Analysis of a large national trauma registry. J Trauma 59:1081–1085
Martin RS, Kilgo PD, Miller PR et al (2005) Injury-associated hypothermia: an analysis of the 2004 National Trauma Data Bank. Shock 24:114–118
Jurkovich GJ, Greiser WB, Luterman A et al (1987) Hypothermia in trauma victims: an ominous predictor of survival. J Trauma 27:1019–1024
Slotman GJ, Jed EH, Burchard KW (1985) Adverse effects of hypothermia in postoperative patients. Am J Surg 149:495–501
Watts DD, Trask A, Soeken K et al (1998) Hypothermic coagulopathy in trauma: effect of varying levels of hypothermia on enzyme speed, platelet function, and fibrinolytic activity. J Trauma 44:846–854
Bernabei AF, Levison MA, Bender JS (1992) The effects of hypothermia and injury severity on blood loss during trauma laparotomy. J Trauma 33:835–839
Ferrara A, MacArthur JD, Wright HK et al (1990) Hypothermia and acidosis worsen coagulopathy in the patient requiring massive transfusion. Am J Surg 160:515–518
Arthurs Z, Cuadrado D, Beekley A et al (2006) The impact of hypothermia on trauma care at the 31st combat support hospital. Am J Surg 191:610–614
Berry JM, Garret K, Clifton GL (1999) Postoperative hypothermia in a tertiary care hospital. Anesthesiology 91:A1177
Gregory JS, Flancbaum L, Townsend MC et al (1991) Incidence and timing of hypothermia in trauma patients undergoing operations. J Trauma 31:795–798; discussion 798–800
Frank SM, Beattie C, Christopherson R et al (1992) Epidural versus general anesthesia, ambient operating room temperature, and patient age as predictors of inadvertent hypothermia. Anesthesiology 77:252–257
Kurz A, Sessler DI, Narzt E et al (1995) Morphometric influences on intraoperative core temperature changes. Anesth Analg 80:562–567
Just B, Trevien V, Delva E et al (1993) Prevention of intraoperative hypothermia by preoperative skin-surface warming. Anesthesiology 79:214–218
Kitamura A, Hoshino T, Kon T et al (2000) Patients with diabetic neuropathy are at risk of a greater intraoperative reduction in core temperature. Anesthesiology 92:1311–1318
Kongsayreepong S, Chaibundit C, Chadpaibool J et al (2003) Predictor of core hypothermia and the surgical intensive care unit. Anesth Analg 96:826–833
Roberts S, Bolton DM, Stoller ML (1994) Hypothermia associated with percutaneous nephrolithotomy. Urology 44:832–835
Garrison JR, Richardson JD, Hilakos AS et al (1996) Predicting the need to pack early for severe intra-abdominal hemorrhage. J Trauma 40:923–927; discussion 927–929
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Inaba, K., Teixeira, P.G.R., Rhee, P. et al. Mortality Impact of Hypothermia After Cavitary Explorations in Trauma. World J Surg 33, 864–869 (2009). https://doi.org/10.1007/s00268-009-9936-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-009-9936-2