
Abstract
Background
Midgut carcinoid (MGC) tumors generally develop in the small intestine and in >50% of cases also present with lymph node metastases in the mesentery. The majority of these tumors are surgically resectable, but a fraction are inoperable and may cause obstruction of the superior mesenteric vein (SMV), often associated with stasis of the intestinal wall and severe symptoms. These symptoms include severe abdominal pain, attacks of diarrhea, and malnutrition.
Methods
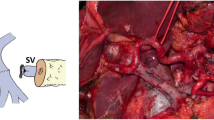
Seven patients with severe MGC including a large fibrotic inoperable mesenteric mass and severe symptoms were studied. After an obstructed SMV and signs of venous stasis in the small intestine were demonstrated, an expandable stent was inserted after puncturing an intrahepatic portal venous branch. The associated venography, patient symptoms, and radiological signs on computed tomography (CT) scans were evaluated.
Results
Four patients demonstrated resolution of their symptoms. In one patient who had intra-abdominal lymph leakage/chyloperitoneum, a complete normalization of the circulation followed and the intra-abdominal lymph leakage stalled. The venographies demonstrated normalization of the venous blood flow through the SMV, and CT scans demonstrated reduction in the thickness of the intestinal wall. In two cases there were no changes in the symptoms, and in one case a slight worsening of the symptoms ensued. In general, reductions of symptoms were associated with the degree of normalization of venous blood flow.
Conclusions
We conclude that in selected patients with MGC stenting of the SMV may improve symptoms.





Similar content being viewed by others


References
Akerstrom G, Hellman P, Hessman O et al (2005) Management of midgut carcinoids. J Surg Oncol 89:161–169
Eriksson B, Kloppel G, Krenning E et al (2008) Consensus guidelines for the management of patients with digestive neuroendocrine tumors–well-differentiated jejunal-ileal tumor/carcinoma. Neuroendocrinology 87:8–19
Hellman P, Lundstrom T, Ohrvall U et al (2002) Effect of surgery on the outcome of midgut carcinoid disease with lymph node and liver metastases. World J Surg 26:991–997
Musunuru S, Chen H, Rajpal S et al (2006) Metastatic neuroendocrine hepatic tumors: resection improves survival. Arch Surg 141:1000–1004 discussion 1005
de Herder WW (2005) Tumours of the midgut (jejunum, ileum and ascending colon, including carcinoid syndrome). Best Pract Res Clin Gastroenterol 19:705–715
Makridis C, Rastad J, Oberg K et al (1996) Progression of metastases and symptom improvement from laparotomy in midgut carcinoid tumors. World J Surg 20:900–906 discussion 907
Åkerström G, Hellman P (2007) Surgery on neuroendocrine tumors. Best Pract Res Clin Endocrinol Metab 21:87–109
Norton J (2005) Surgical treatment of neuroendocrine metastases. Best Pract Res Clin Gastroenterol 19:577–583
Bilbao JI, Ruza M, Longo JM et al (1994) Percutaneous transhepatic stenting by Wallstents of portal vein and bile duct stenoses caused by immunoblastic sarcoma in a liver transplantation. Cardiovasc Intervent Radiol 17:210–213
Harville LE, Rivera FJ, Palmaz JC et al (1992) Variceal hemorrhage associated with portal vein thrombosis: treatment with a unique portal venous stent. Surgery 111:585–590
Kim IH, Kim DG, Kwak HS et al (2008) Ischemic colitis secondary to inferior mesenteric arteriovenous fistula and portal vein stenosis in a liver transplant recipient. World J Gastroenterol 14:4249–4252
Mathias K, Bolder U, Lohlein D et al (1993) Percutaneous transhepatic angioplasty and stent implantation for prehepatic portal vein obstruction. Cardiovasc Intervent Radiol 16:313–315
Olcott EW, Ring EJ, Roberts JP et al (1990) Percutaneous transhepatic portal vein angioplasty and stent placement after liver transplantation: early experience. J Vasc Interv Radiol 1:17–22
Stockland AH, Willingham DL, Paz-Fumagalli R et al (2009) Pancreas transplant venous thrombosis: role of endovascular interventions for graft salvage. Cardiovasc Intervent Radiol 32:279–283
Tanaka J, Andoh H, Yoshioka M et al (2000) Palliative treatment with metallic stents for unresectable gallbladder carcinoma involving the portal vein and bile duct. J Hepatobiliary Pancreat Surg 7:331–335
Wei BJ, Zhai RY, Wang JF et al (2009) Percutaneous portal venoplasty and stenting for anastomotic stenosis after liver transplantation. World J Gastroenterol 15:1880–1885
Vogelzang RL, Reddy SG, Braun MA et al (1996) Extrahepatic portal venous stenosis: treatment with percutaneous transhepatic stent placement. J Vasc Interv Radiol 7:269–271
Yamakado K, Tanaka N, Nakatsuka A et al (1999) Clinical efficacy of portal vein stent placement in patients with hepatocellular carcinoma invading the main portal vein. J Hepatol 30:660–668
Kim YJ, Ko GY, Yoon HK et al (2007) Intraoperative stent placement in the portal vein during or after liver transplantation. Liver Transpl 13:1145–1152
Druce M, Rockall A, Grossman AB (2009) Fibrosis and carcinoid syndrome: from causation to future therapy. Nat Rev Endocrinol 5:276–283
Chiriano J, Teruya TH, Zhang WW et al (2009) Treatment of superior mesenteric artery portal vein fistula with balloon-expandable stent graft. Ann Vasc Surg 23:99–102
Wu CG, Li YD, Li MH (2008) Post-traumatic superior mesenteric arteriovenous fistula: endovascular treatment with a covered stent. J Vasc Surg 47:654–656
Price E, Zukotynski K, Chan R (2008) Endovascular repair of traumatic mesocaval fistula. J Vasc Interv Radiol 19:1659–1661
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hellman, P., Hessman, O., Åkerström, G. et al. Stenting of the Superior Mesenteric Vein in Midgut Carcinoid Disease with Large Mesenteric Masses. World J Surg 34, 1373–1379 (2010). https://doi.org/10.1007/s00268-009-0361-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-009-0361-3