
Abstract
Introduction
A single institutional surgical trial for gastric cancer had demonstrated increased morbidity but not mortality. This report analyzes risk factors affecting morbidity.
Methods
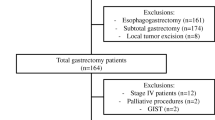
Risk factors for morbidity in 221 patients treated with curative intent were evaluated in a prospective randomized trial comparing D1 and D3 surgery for curable gastric cancer.
Results
The surgeon’s experience after 25 nodal dissections had no influence on surgical or overall complications, nor did the patients’ co-morbidity (e.g., respiratory system disease, cardiac disease, diabetes mellitus). Distal pancreatectomy negatively affected surgical morbidity [relative risk (RR) 6.21, 95% confidence interval (CI) 1.869–20.626] and overall morbidity (RR 5.50, 95% CI 1.671–18.082). All of the patients with a distal pancreatectomy underwent concomitant splenectomy. Multivariate analysis found splenectomy and nodal dissection to be the only two independent risk factors adversely affecting operative morbidity. The RR of splenectomy for surgical complications was 4.19 (95% CI 1.327–13.208), and for overall complications it was 3.88 (95% CI 1.259–11.973). The RR of nodal dissection for surgical complications was 2.51 (95% CI 1.336–4.730), and for overall complications it was 1.93 (95% CI 1.149–3.255).
Conclusions
Splenectomy (with or without pancreatectomy) and nodal dissection are risk factors for operative morbidity but not mortality.
Similar content being viewed by others


References
Pisani P, Parkin DM, Bray F, et al. Estimates of the worldwide mortality from 25 cancers in 1990. Int J Cancer 1999;83:18–29
Taiwan Area: Death Rate of Ten Leading Sites of Malignant Neoplasms, Taiwan, Department of Health, Executive Yuan, 2000;54–62
Wu CW, Lui WY. Current management of gastric cancer in Taiwan. Asian J Surg 2001;48:253–257
Cady B. Lymph node metastases: indicators, but not governors of survival. Arch Surg 1984;119:1067–1072
Bonenkamp JJ, Songun I, Hermans J, et al. Randomised comparison of morbidity after D1 and D2 dissection for gastric cancer in 996 Dutch patients. Lancet 1995;345:745–748
Cuschieri A, Fayers P, Fielding J, et al. Post-operative morbidity and mortality after D1 and D2 resections for gastric cancer: preliminary results of the MRC randomized controlled surgical trial. Lancet 1996;347:995–999
Sasako M. Risk factors for surgical treatment in the Dutch gastric cancer trial. Br J Surg 1997;84:1567–1571
Smith JM, Shiu MH, Kelsey L, et al. Morbidity of radical lymphadenectomy in the curative resection of gastric carcinoma. Arch Surg 1991;126:1469–1473
Roder JD, Bottcher K, Siewert JR, et al. Prognostic factors in gastric carcinoma: results of the German Gastric Carcinoma study. Cancer 1993;72:2089–2097
Heslin MJ. Extended lymph node dissection in gastric cancer: if a benefit exists, can it ever be proven? Ann Surg Oncol 2000;7:715–716
Wu CW, Hsiung CA, Lo SS, et al. Randomized clinical study of morbidity after D1 and D3 surgery for gastric cancer. Br J Surg 2004;91:283–287
Japanese Research Society for Gastric Cancer. Japanese Classification of Gastric Carcinoma, 1st English edition, Tokyo, Kanehara, 1995
Wu CW, Hsieh MC, Lo SS, et al. Morbidity and mortality after radical gastrectomy for patients with carcinoma of the stomach. J Am Coll Surg 1995;181:26–32
Lo SS, Wu CW, Shen KH, et al. Higher morbidity and mortality after combined total gastrectomy and pancreaticosplenectomy for gastric cancer. World J Surg 2002;26:678–682
Wu CW, Chen Y, Hsieh MJ, et al. Use of a modified Foley catheter for continuous irrigation of intra-abdominal abscess. Br J Surg 1992;79:1296
Csendes A, Burdiles P, Rojas J, et al. A prospective randomized study comparing D2 total gastrectomy versus D2 total gastrectomy plus splenectomy in 187 patients with gastric carcinoma. Surgery 2002;131:401–407
Acknowledgements
The authors thank Hui-Tzu Yu and Yurh-Ling Ho of the data center at the National Health Research Institutes and research nurse Li-Ting Shia for assistance with data collection and processing. This study was supported by the Division of Cancer Research, National Health Research Institutes, Taiwan.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wu, CW., Chang, IS., Lo, Ss. et al. Complications Following D3 Gastrectomy: Post Hoc Analysis of a Randomized Trial. World J. Surg. 30, 12–16 (2006). https://doi.org/10.1007/s00268-005-7951-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-005-7951-5