
Abstract
Background
Parathyroid exploration through a standard cervical approach is adequate for the resection of most mediastinal parathyroid glands. A subset of mediastinal parathyroid glands causing hyperparathyroidism, however, cannot be removed in this manner.
Study Design
We reviewed our experience with the use of partial median sternotomy in the treatment of these patients.
Results
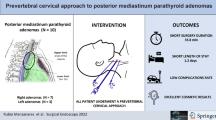
Over a 14-year period, all but 10 of 937 (1.1%) consecutive patients explored for hyperparathyroidism by a single endocrine surgeon were treated by a cervical approach. Partial median sternotomy was performed in 10 cases and was successful in seven cases (70%), with conversion to a complete sternotomy being required in three cases. Six of these seven patients had failed a previous parathyroid exploration (86%), including one patient who had a previous complete sternotomy. Cure of hyperparathyroidism was achieved in all seven patients undergoing partial median sternotomy. In five patients a mediastinal parathyroid gland was removed (71%), and in one patient a parathyroid adenoma in the carotid sheath was eventually found, and the location of the hyperfunctioning parathyroid gland in one patient was never determined although the patient was cured. The mean length of hospital stay after a partial median sternotomy was 2.6 days. One patient sustained a recurrent laryngeal nerve injury at the time of a repeat cervical exploration and partial median sternotomy.
Conclusions
Rarely, mediastinal parathyroid glands cannot be resected through a cervical approach. In these cases the use of partial median sternotomy is an attractive technique in achieving cure of hyperparathyroidism and is associated with minimal morbidity and a short length of hospital stay.




Similar content being viewed by others


References
Bauer W, Federman DD. Hyperparathyroidism epitomized: the case of Captain Charles E. Martell. Metabolism 1962;11:21–29
Wang CA. The anatomic basis of parathyroid surgery. Ann Surg 1976;183:271–275
Kurtay M, Crile G Jr. Aberrant parathyroid glands in relationship to the thymus. Am J Surg 1969;117:705
Wells SA Jr, Leight GS, Ross AJ 3rd. Primary hyperparathyroidism. Curr Probl Surg 1980;17:398–463
Edis AJ, Sheedy PF, Beahrs OH, et al. Results of reoperation for hyperparathyroidism, with evaluation of preoperative localization studies. Surgery 1978;84:384–393
van Vroonhoven TJ, Muller H. Causes of failure in the surgical treatment of primary hyperparathyroidism: lessons from 51 successful reoperations. Br J Surg 1978;65:297–300
Nudelman IL, Deutsch AA, Reiss R. Primary hyperparathyroidism due to mediastinal parathyroid adenoma. Int Surg 1987;72:104–108
Clark OH. Mediastinal parathyroid tumors. Arch Surg 1988;123:1096–1100
Conn JM, Goncalves MA, Mansour KA, et al. The mediastinal parathyroid. Am Surg 1991;57:62–66
Cupisti K, Dotzenrath C, Simon D, et al. Therapy of suspected intrathoracic parathyroid adenomas. Experiences using open transthoracic approach and video-assisted thoracoscopic surgery. Langenbecks Arch Surg 2002;386:488–493
Rothmund M, Diethelm L, Brünner H, et al. Diagnosis and surgical treatment of mediastinal parathyroid tumors. Ann Surg 1976;183:139–145
Roslyn JJ, Gordon HE, Mulder DG. Mediastinal parathyroid adenomas. A cause of persistent hyperparathyroidism. Am Surg 1983;49:523–527
Wang CA, Gaz RD, Moncure AC. Mediastinal parathyroid exploration: a clinical and pathologic study of 47 cases. World J Surg 1986;10:687–695
Schlinkert RT, Whitaker MD, Argueta R. Resection of select mediastinal parathyroid adenomas through an anterior mediastinotomy. Mayo Clin Proc 1991;66:1110–1113
Doherty GM, Doppman JL, Miller DL, et al. Results of a multidisciplinary strategy for management of mediastinal parathyroid adenoma as a cause of persistent primary hyperparathyroidism. Ann Surg 1992;215:101–106
Kido T, Hazama K, Inoue Y, et al. Resection of anterior mediastinal masses through an infrasternal approach. Ann Thorac Surg 1999;67:263–265
Medrano C, Hazelrigg SR, Landreneau RJ, et al. Thoracoscopic resection of ectopic parathyroid glands. Ann Thorac Surg 2000;69:221–223
Miller JI, Mansour KA, Hatcher CR Jr. Median sternotomy T incision for thymectomy in myasthenia gravis. Ann Thorac Surg 1982;34:473–474
Grandjean JG, Lucchi M, Mariani MA. Reversed-T upper mini-sternotomy for extended thymectomy in myasthenic patients. Ann Thorac Surg 2000;70:1423–1424
Paletto AE, Maggi G. Thymectomy in the treatment of myasthenia gravis: results in 320 patients. Int Surg 1982;67:13–16
LoCicero J 3rd. The combined cervical and partial sternotomy approach for thymectomy. Chest Surg Clin N Am 1996;6:85–93
Pego-Fernandes PM, de Campos JR, Jatene FB, et al. Thymectomy by partial sternotomy for the treatment of myasthenia gravis. Ann Thorac Surg 2002;74:204–208
Orringer MB. Partial median sternotomy: anterior approach to the upper thoracic esophagus. J Thorac Cardiovasc Surg 1984;87:124–129
Konertz W, Waldenberger F, Schmutzler M, et al. Minimal access valve surgery through superior partial sternotomy: a preliminary study. J Heart Valve Dis 1996;5:638–640
Szwerc MF, Benckart DH, Wiechmann RJ, et al. Partial versus full sternotomy for aortic valve replacement. Ann Thorac Surg 1999;68:2209–2213
Masiello P, Coscioni E, Panza A, et al. Surgical results of aortic valve replacement via partial upper sternotomy: comparison with median sternotomy. Cardiovasc Surg 2002;10:333–338
Dogan S, Dzemali O, Wimmer-Greinecker G, et al. Minimally invasive versus conventional aortic valve replacement: a prospective randomized trial. J Heart Valve Dis 2003;12:76–80
Russell CF, Edis AJ, Scholz DA, et al. Mediastinal parathyroid tumors: experience with 38 tumors requiring mediastinotomy for removal. Ann Surg 1981;193:805–809
Norton JA, Schneider PD, Brennan MF. Median sternotomy in reoperations for primary hyperparathyroidism. World J Surg 1985;9:807–813
Gaz RD, Doubler PB, Wang CA. The management of 50 unusual hyperfunctioning parathyroid glands. Surgery 1987;102:949–957
Wells SA Jr., Cooper JD. Closed mediastinal exploration in patients with persistent hyperparathyroidism. Ann Surg 1991;214:555–561
McNeill TM, Chamberlain JM. Diagnostic anterior mediastinotomy. Ann Thorac Surg 1966;2:532–539
Wang CA. Parathyroid re-exploration. A clinical and pathological study of 112 cases. Ann Surg 1977;186:140–145
Granberg PO, Johansson G, Lindvall N, et al. Reoperation for primary hyperparathyroidism. Am J Surg 1982;143:296–300
Acknowledgments
The authors are grateful to Juan R. Garcia, Certified Medical Illustrator, for his artistic contributions.
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented in part at the Society of Surgical Oncology 57th Annual Cancer Symposium, New York, NY, March 18–21, 2004
Rights and permissions
About this article
Cite this article
Gold, J.S., Donovan, P.I. & Udelsman, R. Partial Median Sternotomy: An Attractive Approach to Mediastinal Parathyroid Disease. World J. Surg. 30, 1234–1239 (2006). https://doi.org/10.1007/s00268-005-7904-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-005-7904-z