
Abstract
Introduction
The resectability rate and postoperative survival rate for pancreatic carcinoma are poor. Aggressive resection including vascular resection and extended lymphadenectomy represent one strategy for improving survival. This study was carried out to clarify the indications for extended resection, especially vascular resection, for pancreatic carcinoma.
Methods
From July 1981 to March 2005, we performed curative resection in 289 of 443 patients with pancreatic carcinoma in our department (65.2%). Vascular resection was performed in 201 (69.5%) patients and portal vein resection without arterial resection in 186 patients. Combined portal and arterial resection was performed in 14 patients and arterial resection without portal vein resection in 1. Extended lymphadenectomy including paraaortic lymph nodes was done. The postoperative survival rate was stratified according to operative and pathology findings.
Results
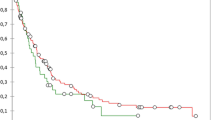
Operative mortality (any death within 30 days after surgery) occurred in 11 of the 289 curative resection patients (3.8%), including 1 of 88 patients without vascular resection (1.1%), 5 of 186 portal vein resection patients without arterial resection (2.7%), and 5 of 14 (35.7%) arterial resection patients undergoing portal vein arterial resection as well. Most patients who survived for 2 to 3 years had carcinoma-free surgical margins.
Conclusions
The most important indication for vascular resection in patients with pancreatic cancer is the ability to obtain cancer-free surgical margins. Otherwise, vascular resection is contraindicated. Extended lymphadenectomy may be not of benefit.









Similar content being viewed by others


References
Japan Pancreas Society. National Pancreatic Cancer Registry, Japan: a report of 20 years. Suizo (J Jpn Pancreat Soc) 2003;18:101–169 (in Japanese)
Fortner JG. Regional resection of cancer of the pancreas: a new surgical approach. Surgery 1973;73:307–320
Nakao A, Horisawa M, Suenaga M, et al. Temporal portosystemic bypass with the use of the heparinized hydrophilic catheter. Jpn J Artif Organs 1982;11:962–965
Nakao A, Hirosawa M, Kondo T, et al. Total pancreatectomy accompanied by portal vein resection using catheter–bypass of the portal vein. Shujutsu (Operation) 1983;37:1–6 (in Japanese)
Nakao A, Nonami T, Harada A, et al. Portal vein resection with a new antithrombogenic catheter. Surgery 1990;108:913–918
Nakao A, Takagi H. Isolated pancreatectomy for pancreatic head carcinoma using catheter-bypass of the portal vein. Hepatogastroenterology 1993;40:426–429
Japan Pancreas Society. Classification of Pancreatic Carcinoma, 2nd English edition. Tokyo, Kanehara, 2003
Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958;53:457–481
Nakao A, Ichihara T, Nonami T, et al. Clinicohistopathologic and immunohistochemical studies of intrapancreatic development of carcinoma of the head of the pancreas. Ann Surg 1989;209:181–187
Ichihara T, Nakao A, Suzuki Y, et al. Improvement of the rapid immunoperoxidase staining method for intraoperative pathological diagnosis of pancreatic cancer using microwave irradiation. J Surg Oncol 1989;42:209–214
Nakao A, Harada A, Nonami T, et al. Lymph node metastasis in carcinoma of the head of the pancreas region. Br J Surg 1995;82:399–402
Nakao A, Harada A, Nonami T, et al. Lymph node metastasis in carcinoma of the body and tail of the pancreas. Br J Surg 1997;84:1090–1092
Ishikawa O, Ohhigashi H, Sasaki Y, et al. Practical usefulness of lymphatic and connective tissue clearance for the carcinoma of the pancreas head. Ann Surg 1988;208:215–220
Kayahara M, Nagakawa T, Ueno K, et al. Surgical strategy for carcinoma of the pancreas head area based on clinicopathologic analysis of nodal involvement and plexus invasion. Surgery 1995;117:616–623
Sakai M, Nakao A, Kaneko T, et al. Para–aortic lymph node metastasis in carcinoma of the head of the pancreas. Surgery 2005;137:606–611
Fortner JG, Klimstra DS, Senie RT, et al. Tumor size is the primary prognosticator for pancreatic cancer after regional pancreatectomy. Ann Surg 1996;223:147–153
Pedrazzoli S, DiCarlo V, Dionigi R, et al. Standard versus extended lymphadenectomy associated with pancreaticoduodenectomy in the surgical treatment of adenocarcinoma of the head of the pancreas: a multicenter, prospective, randomized study. Ann Surg 1998;228:508–517
Yeo CJ, Cameron JK, Lillemoe KD, et al. Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma. Part 2. Randomized controlled trial evaluating survival, morbidity, and mortality. Ann Surg 2002;236:355–368
Nakao A, Harada A, Nonami T, et al. Clinical significance of carcinoma invasion of the extrapancreatic nerve plexus in pancreatic cancer. Pancreas 1996;12:357–361
Kaneko T, Nakao A, Inoue S, et al. Intraportal endovascular ultrasonography in the diagnosis of portal vein invasion by pancreatobiliary carcinoma. Ann Surg 1995;222:711–718
Nakao A, Kaneko T. Intravascular ultrasonography for assessment of portal vein invasion by pancreatic cancer. World J Surg 1999;23:892–895
Kaneko T, Nakao A, Inoue S, et al. Extrapancreatic nerve plexus invasion by carcinoma of the head of the pancreas: diagnosis with intraportal endovascular ultrasonography. Int J Pancreatol 1996;19:1–7
Nakao A, Harada A, Nonami T, et al. Clinical significance of portal invasion of carcinoma of the head of the pancreas. Surgery 1995;117:50–55
Nakao A, Takeda S, Sakai M, et al. Extended radical resection versus standard resection for pancreatic cancer: the rationale for extended radical resection. Pancreas 2004;28:289–292
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nakao, A., Takeda, S., Inoue, S. et al. Indications and Techniques of Extended Resection for Pancreatic Cancer. World J. Surg. 30, 976–982 (2006). https://doi.org/10.1007/s00268-005-0438-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-005-0438-6