
Abstract
Background
Anesthesia adversely affects respiratory function and hemodynamics in obese patients. Although many studies have been performed in morbidly obese patients, data are limited concerning overweight patients [BMI 25–29.9 kg m−2]. The aim of this study was to evaluate the effects of prolonged pneumoperitoneum in Trendelenburg position on hemodynamics and gas exchange in normal and overweight patients.
Methods
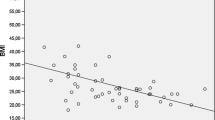
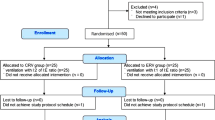
We studied 15 overweight and 15 non-obese [BMI 18.5–24.9 kg m−2] patients who underwent totally endoscopic robot-assisted radical prostatectomy under general anesthesia with an inspired oxygen fraction of 0.5. A standardized anesthetic regimen was used, and patients were examined at standard times: after induction of anesthesia and Trendelenburg posture, every 30 minutes after establishing pneumoperitoneum, and after the release of the pneumoperitoneum with the patient still in Trendelenburg position.
Results
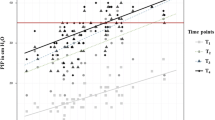
After induction of anesthesia and Trendelenburg positioning arterial oxygen pressure [PaO2] and alveolar-arterial difference in oxygen tension [AaDO2] differed significantly between both groups with lower PaO2 [235 ± 27 versus 164 ± 51 mmHg] and higher AaDO2 [149 ± 48 versus 76 ± 28 mmHg] values in overweight patients. During pneumoperitoneum, PaO2 transient increased above baseline values in overweight patients, whereas AaDO2 decreased. Hemodynamic parameters [HR, MAP, and CVP] did not differ significantly between groups.
Conclusions
Arterial oxygenation and AaDO2 are significantly impaired in overweight patients under general anesthesia in Trendelenburg posture. In overweight patients pneumoperitoneum transient reduced the impairment of arterial oxygenation and lead to a decrease in AaDO2. Hemodynamic parameters were not affected by body weight.



Similar content being viewed by others
References
Kuczmarski RJ, Flegal KM, Campell SM, et al. Increasing prevalence of overweight among U.S. adults: The National Health and Nutrition Surveys, 1960–1991. J Am Med Assoc 1994;272:205–211
Luce JM. Respiratory complications of obesity. Chest 1980;78:626–631
Tokics L, Hedenstierna G, Strandberg A, et al. Lung collapse and gas exchange during general anesthesia: effects of spontaneous breathing, muscle paralysis, and positive end-expiratory pressure. Anesthesiology 1987;66:157–167
Safran DB, Orlando R. Physiologic effects of pneumoperitoneum. Am J Surg 1994;167:281–286
Nishio I, Noguchi J, Konishi M, et al. The effects of anesthetic techniques and insufflating gases on ventilation during laparoscopy. Masui 1993;42:862–866
Fahy BG, Barnas GM, Flowers JL, et al. The effects of increased abdominal pressure on lung and chest wall mechanics during laparoscopic surgery. Anesth Analg 1995;81:744–750
Fahy BG, Barnas GM, Nagle SE, et al. Effects of Trendelenburg and reverse Trendelenburg postures on lung and chest wall mechanics. J Clin Anesth 1996;8:236–244
Wahba RW. Perioperative functional residual capacity. Can J Anaesth 1991;38:938–939
Barnas GM, Green MD, Mackenzie CF, et al. Effect of posture on lung and regional chest wall mechanics. Anesthesiology 1993;78:251–259
Allen SJ, Tonnesen AS. Advances respiratory life support. In Hoyt JW, Tonnesen AS, Allen SJ, editors, Critical Care Practice, Philadelphia, WB Saunders, 1991;49–80
Acknowledgments
We thank Gerhard Vogt, MD, for his laboratory work and support during the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Meininger, D., Zwissler, B., Byhahn, C. et al. Impact of Overweight and Pneumoperitoneum on Hemodynamics and Oxygenation during Prolonged Laparoscopic Surgery. World J. Surg. 30, 520–526 (2006). https://doi.org/10.1007/s00268-005-0133-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-005-0133-7