
Abstract
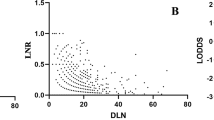
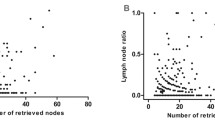
In patients with squamous cell carcinoma of the esophagus, the preoperative clinical staging of the N category is primarily based on the lymph node size. Lymph nodes >10 mm are considered to be tumor-infiltrated. This histopathologic study investigated the correlation of lymph node size and metastatic infiltration in esophageal carcinoma of patients with and without neoadjuvant radiochemotherapy. The specimens of 40 patients with squamous cell carcinoma of the esophagus were included in a prospective morphometric study. Half of these patients (n=20) received preoperative radiochemotherapy. The number of resected lymph nodes were counted, and the largest diameter of each node was measured. Metastatic involvement of each node was analyzed by histologic examination. The frequency of lymph node metastases was calculated and correlated to the lymph node size. A total of 1196 lymph nodes with an average of 29.9 nodes per patient were resected and analyzed; 129 lymph nodes (10.8%) showed metastatic infiltration. The average size of 1067 tumor-free lymph nodes was 5.1±3.8 mm in maximum diameter, whereas the average size of 129 metastatic lymph nodes was 6.7±4.2 mm (p=0.00006). Of all resected lymph nodes, 761 (63.6%) were ≤5 mm in maximum diameter. Only 9.3% (n=111) of all resected lymph nodes were >10 mm in maximum diameter. There was no significant correlation between lymph node size and the frequency of nodal metastases. No difference in size could be demonstrated between patients with and without neoadjuvant radiochemotherapy. Diagnostic imaging techniques using size as the criterion of nodal infiltration cannot exactly assess the nodal status of patients with esophageal carcinoma. This is also true for patients after neoadjuvant radiochemotherapy. Therefore, evaluation of the nodal status in patients with squamous cell carcinoma of the esophagus is entirely based on pathohistologic analysis after a well defined lymphadenectomy.
Résumé
Chez les patients porteurs d’un cancer épidermoïde de l’oesophage, le staging clinique préopératoire de l’état lymphatique est basé principalement sur la taille ganglionnaire: toute adénopathie de taille supérieure à 10 mm est considérée comme tumorale. Dans cette étude histopathologique, on examine la corrélation entre la taille des ganglions et l’infiltration métastatique de l’œsophage chez les patients porteurs de cancer de l’œsophage avec ou sans radiochimiothérapie néoadjuvante. On a réalisé une étude prospective morphologique sur 40 pièces provenant de patients porteurs de cancer épidermoïde de l’œsophage: 20 ayant eu une radiochimiothérapie préopératoire. On a compté le nombre de ganglions lymphatiques et a mesuré le diamètre le plus important de chaque ganglion. L≐envahissement métastatique a été déterminé par l’examen histologique. On a calculé la fréquence des métastases ganglionnaires, corrélée ensuite à la taille ganglionnaire. On a réséqué et analysé au total 1196 ganglions avec une moyenne de 29.9 ganglions par patient. On a trouvé une infiltration métastatique dans 129 ganglions (10.8%). Le diamètre maximal des 1067 ganglions sans tumeur a été de 5.1±3.8 mm alors que celui des 129 ganglions métastatiques a été de 6.7±4.2 mm (p=0.00006). 761 de tous les ganglions réséqués (63.6%) avaient un diamètre maximal de 5 mm ou moins. 93% (111 ganglions lymphatiques) de tous les ganglions réséqués avaient un diamètre maximal de plus de 10 mm. On n’a noté aucune différence statistiquement significative entre la taille ganglionnaire et la fréquence des métastases ganglionnaires. On n’a retrouvé aucune différence statistiquement significative entre les patients ayant eu une radiochimiothérapie néoadjuvante ou pas. Les techniques d’imagerie diagnostique utilisant la taille comme critère d’infiltration néoplasique ne peuvent être utilisées pour préciser l’état ganglionnaire des patients porteurs de cancer de l’œsophage. Ceci est également vrai pour les patients après radiochimiothérapie néoadjuvante. Ainsi, l’évaluation de l’état ganglionnaire des patients porteurs de cancer épidermoïde de l’œsophage est entièrement basée sur l’analyse histopathologique après un curage ganglionnaire bien défini.
Resumen
En pacientes con carcinoma de células escamosas de esófago la estadificación clínica preoperatoria de la categoría N se fundamenta principalmente en el tamaño de los ganglios linfáticos. Cuando éstos son mayores de 10 mm se considera que están metastatizados. Este estudio histopatológico trata de averiguar si existe o no una correlación entre el tamaño de los ganglios linfáticos y su metastatización en pacientes con carcinoma esofágico tratados con o sin radioquimioterapia neoadyuvante. En este estudio prospectivo morfométrico se incluyeron las piezas operatorias correspondientes a 40 pacientes con carcinoma de células escamosas del esófago, de los que 20 correspondían a pacientes que recibieron radioquimioterapia preoperatoria. Se realizó un recuento de las adenopatías resecadas, midiéndose el diámetro mayor de cada una de ellas. Se examinó histológicamente el grado de infiltración metastásica de cada ganglio. La frecuencia de metástasis ganglionares se calculó y correlacionó con el tamaño del ganglio linfático. En total se resecaron y analizaron 1196 ganglios linfáticos con una media por paciente de 29.9. En 129 ganglios (10.8%) se constató infiltración metástasica. El diámetro máximo de los 1067 ganglios no metastatizados fue de 5.1±3.8 mm, mientras que el de los 129 metastatizados fue de 6.7±4.2 mm (p=0.00006). 761 de todas las adenopatias resecadas (63.6%) presentaban un diámetro igual o menor a los 5 mm. Solo el 9.3% (111 ganglios) de las adenopatías resecadas tenían un diámetro máximo mayor de 10 mm. No registramos correlación significativa entre el tamaño del ganglio y la incidencia metastásica. Tampoco se observó diferencia alguna, por lo que al tamaño se refiere, entre ganglios obtenidos de pacientes tratados con o sin radioquimioterapia neoadyuvante. Las técnicas de diagnóstico que se basan en el tamaño de las adenopatías para establecer un criterio de metastatización ganglionar no son exactas ni correctas para la valoración de la estadificación del carcinoma esofágico. De ahí, que la evaluación de la estadificación ganglionar en pacientes con carcinoma de células escamosas del esófago haya de basarse, exclusivamente, en el análisis histopatológico tras una linfadenectomía amplia.
Similar content being viewed by others

References
Roder JD, Busch R, Stein HJ, et al. Ratio of invaded to removed lymph nodes as a predictor of survival in squamous cell carcinoma of the oesophagus. Br. J. Surg. 1994;81:410–413
Hölscher AH, Bollschweiler E, Bumm R, et al. Prognostic factors of resected adenocarcinoma. Surgery 1995;118:845–855
Hölscher AH, Dittler HJ, Siewert JR. Staging of squamous esophageal cancer: accuracy and value. World J. Surg. 1994;18:312–320
Takashima S, Takeuchi N, Shiozaki K, et al. Carcinoma of the esophagus: CT vs MR imaging in determining resectability. A.J.R. Am. J. Roentgenol. 1991;156:297–302
Botet JF, Lightdale CJ, Zauber AG, et al. Preoperative staging of esophageal cancer: comparison of endoscopic US and dynamic CT. Radiology 1991;181:419–425
Dworak O. Number and size of lymph nodes and node metastases in rectal carcinomas. Surg. Endose. 1989;3:96–99
Kerr M, Lamb D, Wathen CG. Pathological assessment of mediastinal lymph nodes in lung cancer: implications for noninvasive mediastinal staging. Thorax 1992;47:337–341
Noda N, Sasako M, Yamaguchi N, et al. Ignoring small lymph nodes can be a major cause of staging error in gastric cancer. Br. J. Surg. 1998;85:831–834 10.1046/j. 1365-2168.1998.00691.x
Mönig SP, Zirbes TK, Schröder W, et al. Staging of gastric cancer: correlation of lymph node size and metastatic infiltration. A.J.R. Am. J. Roentgenol. 1999;173:365–367
Mönig SP, Baldus S, Zirbes T, et al. Lymph node size and metastatic infiltration in colon cancer. Ann. Surg. Oncol. 1999;6:579–581
Siewert JR, Bartels H, Bollschweiler E. Plattenepithelcarcinom des Ösophagus: Behandlungskonzepte der Chirurgischen Klinik der Technischen Universität München. Chirurg 1992;63:693–700
Sobin LH, Wittekind C, editors. UICC. TNM Classification of Malignant Tumors, 5th edition, New York, Wiley, 1997;54–58
Siewert JR, Fink U. Multimodale Therapiekonzepte bei Tumoren des Gastrointestinaltraktes. Chirurg 1992;63:242–250
Bosset JF, Gignoux M, Triboulet J-P, et al. Chemotherapy followed by surgery compared with surgery alone in squamous-cell cancer of the esophagus. N. Engl. J. Med. 1997;337:161–167
Siewert JR, Dittler HJ. Esophageal carcinoma: impact of staging on treatment. Endoscopy 1993;25:28–32
Catalano MF, Sivak MV, Rice T, et al. Endosonographie features predictive of lymph node metastasis. Gastrointest. Endose. 1994;40: 442–446
Chandawarkar RY, Kakegawa T, Fujita H, et al. Endosonography for preoperative staging of specific nodal groups associated with esophageal cancer. World J. Surg. 1996;20:700–702
Flanagan FL, Dehdashti F, Siegel BA, et al. Staging of esophageal cancer with 18F-fluorodeoxyglucose positron emission tomography. A.J.R. Am. J. Roentgenol. 1997;168:417–424
Author information
Authors and Affiliations
Corresponding author
Additional information
Published Online: February 12, 2002
Rights and permissions
About this article
Cite this article
Schröder, W., Baldus, S.E., Mönig, S.P. et al. Lymph node staging of esophageal squamous cell carcinoma in patients with and without neoadjuvant radiochemotherapy: Histomorphologic analysis. World J. Surg. 26, 584–587 (2002). https://doi.org/10.1007/s00268-001-0271-5
Issue Date:
DOI: https://doi.org/10.1007/s00268-001-0271-5