
Abstract
Purpose
The authors made a retrospective analysis of three triage situations of war wounded in Chad and Rwanda in which mass casualties overwhelmed available medical facilities.
Methods
The triage classification is based on the waiting period for surgery. The categories are: extreme, first, second and third emergencies, expectant, walking wounded.
Results
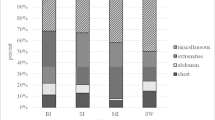
In Chad, 23 wounded adults were received in 24 hours, and 19 were operated up on within 48 hours. In Rwanda 1, 94 wounded were received in two hours, of whom 68 were operated upon, 23 on the first day. In Rwanda 2, 59 wounded were received in 12 hours, treatment of extreme and first emergencies required 48 hours, while second and third emergencies were treated during the three following days.
Conclusions
These episodes were very different when considering the setting, the number of casualties, the type of wounds, the logistical and medical difficulties. The authors report the difficulties faced and the lessons learned.
“Il faut toujours commencer par le plus douloureusement blessé sans avoir égard aux rangs et aux distinctions.” You must always begin with those who are most seriously wounded without regard to rank or other distinction. Baron Larrey (1766–1842), surgeon to Napoléon’s Imperial Guard [1]




Similar content being viewed by others


References
Larrey DJ (1984) Mémoires et campagnes du baron Larrey. Campagnes de Saxe et de Prusse. Première réédition, Remanences Editions, Paris, p 4
Blair JSG (2005) Famous figures: James Dominique, First Baron Larrey. J R Army Med Corps 151:207–208
Morris JA Jr, Auerbach PS, Marshall GA et al (1986) The trauma score as a triage tool in the prehospital setting. JAMA 256(10):319–325
Burris DG, Fitz-Harris JB, Holcomb JB et al (2004) Emergency war surgery. US Government Printing Office, Washington DC
Giannou C, Baldan M (2009) War surgery working with limited resources in armed conflict and other situations of violence, vol 1, chap 9. Hospital triage of mass casualties. International Committee of the Red Cross, March 2009
Burkle FM Jr, Newland C, Orebaugh S, Blood CG (1994) Emergency medicine in the Persian Gulf War-Part 2. Triage : methodology and lessons learned. Ann Emerg Med 23(4):748–754
Houdelette P (1996) Le triage de blessés de guerre en chirurgie de guerre et en situation d’exception. J Chir (Paris) 133(8):363–712
Coupland RM, Parker PJ, Gray RC (1992) Triage of war wounded: the experience of the International Committee of the Red Cross. Injury 23(8):507–510
Coupland RM (1994) Epidemiological approach to surgical management of the casualties of war. BMJ 308(6945):1693–1697
Cone DC, Serra J, Burns K, MacMillan DS, Kurland L, Van Gelder C (2009) Pilot test of the SALT Mass Casualty Triage System. Prehosp Emerg Care 13(4):536–540
Domres B, Koch M, Manger A, Becker HD (2001) Ethics and triage. Prehosp Disaster Med 16(1):53–58
Frykberg ER (2005) Triage: principles and practice. Scand J Surg 94:272–278
Adu-Gyamfi Y (1997) The Gulf War: the experience of a department of anesthesiology in the management of Scud missile casualties. Prehosp Disaster Med 12(2):109–113
International Red Cross (1995) Convention (IV) Relative to the Protection of Civilian Persons in Time of War. Geneva, 12 August 1949. Part II. General protection of populations against certain consequences of war. Art. 13. International Humanitarian Law—Treaties & Documents. International Committee of the Red Cross, Geneva, ref 0173, p 245
Conflict of interest
The authors declare that they have no conflict of interest.
The views expressed are solely those the authors and do not necessary reflect the official policy or position of the French army medical service.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rigal, S., Pons, F. Triage of mass casualties in war conditions: realities and lessons learned. International Orthopaedics (SICOT) 37, 1433–1438 (2013). https://doi.org/10.1007/s00264-013-1961-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-013-1961-y