
Abstract
Background
Given the fact that prostate cancer incidence will increase in the coming years, new prognostic biomarkers are needed with regard to the biological aggressiveness of the prostate cancer diagnosed. Since cytokines have been associated with the biology of cancer and its prognosis, we determined whether transforming growth factor beta 1 (TGFβ1), interleukin-7 (IL-7) receptor and IL-7 levels add additional prognostic information with regard to prostate cancer-specific survival.
Materials and methods
Retrospective survival analysis of forty-four prostate cancer patients, that underwent radical prostatectomy, was performed (1989–2001). Age, Gleason score and pre-treatment PSA levels were collected. IL-7, IL-7 receptor and TGFβ1 levels in prostate cancer tissue were determined by quantitative real-time RT-PCR and their additional prognostic value analyzed with regard to prostate cancer survival. Hazard ratios and their confidence intervals were estimated, and Akaike’s information criterion was calculated for model comparison.
Results
The predictive ability of a model for prostate cancer survival more than doubled when TGFβ1 and IL-7 were added to a model containing only the Gleason score and pre-treatment PSA (AIC: 18.1 and AIC: 6.5, respectively).
Conclusion
IL-7 and TGFβ1 are promising markers to indicate those at risk for poor prostate cancer survival. This additional information may be of interest with regard to the biological aggressiveness of the diagnosed prostate cancer, especially for those patients screened for prostate cancer and their considered therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
According to UN Projections, the population aged 60 or over increases from 475 million in 2009 to 1.6 billion in the year 2050. Since prostate cancer is primarily a disease of elderly males, one could expect an increase of prostate cancer incidence in the coming years. In addition, an extra increase could be expected as a consequence of screening for prostate cancer, for example, using prostate-specific antigen (PSA) [1, 2].
Histologic tumor grading of prostate cancer is essential for the assessment of prognosis. Prognosis refers to the expected biologic potential of a patient’s prostate cancer to spread to other organs, that is, to metastasize. Prognosis is, among others, based upon PSA pre-treatment level and the Gleason score. The Gleason grading system uses the histological pattern of neoplastic cells in hematoxylin-eosin-stained sections and is largely subjectively scored by the pathologist [3].
Gleason scores can be derived from both biopsy and radical prostatectomy samples. The biopsy-derived Gleason score often undergrades the Gleason score of the actual tumor because of sampling error [4–6]. Furthermore, a high variability has been described in the way clinicians use prostate needle biopsy-based pathology reports [7–9]. Despite the inter and intraobserver variabilities of Gleason score determination, and discordance in the Gleason score between biopsy and radical prostatectomy specimens, the Gleason score remains the most important prognostic factor for prostate cancer clinical outcome and therefore strongly influences decisions regarding options for therapy [4–6, 10, 11]. The above limitations of the Gleason score indicate the need for additional, and preferably objectively measured information on the biological aggressiveness of the diagnosed prostate cancer, especially while screening for prostate cancer.
Cytokines have been associated with the biology of cancer and its prognosis. These low molecular weight molecules have significant roles, not only in immune/inflammatory systems, but also in hematopoiesis, the acute phase response, and multiple other functions. Specific cytokines have been found to be elevated in plasma of patients with various malignancies including prostate cancer. For example, earlier studies suggested a relation between increased levels of interleukin-4 (IL-4), IL-6 and IL-10 with prostate malignancy [12, 13]. Other studies reported patients with metastatic prostate cancer which were associated with increased transforming growth factor beta (TGFβ) serum levels, and TGFβ1 accumulation in primary and metastatic prostate cancer tissue samples [14–18]. Furthermore, an antagonistic relationship has been suggested for TGFβ and IL-7. TGFβ down regulates IL-7 secretion [19], whereas IL-7 inhibits the production of TGF-beta1 by tumor cells [20].
In non-cancer cells, TGFβ stops cell proliferation, induces differentiation, or promotes apoptosis. In cancer cells, mutations of the TGFβ pathway confer resistance to growth inhibition by TGFβ, resulting in uncontrolled cell proliferation. The increase of TGFβ production in cancer cells also stimulates angiogenesis and suppresses the activities of infiltrating immune cells, thereby facilitating the tumor to escape immunosurveillance [21]. On the other hand, IL-7 promotes T cell cytolytic, innate responses, antitumor reactivity in lung cancer, and prolonged survival in mice after whole cell vaccination with cells that are able to secrete mIL-7 [22–25]. Loss of epithelial IL-7 in prostate cancer tissue is associated with a severe depletion of prostate-associated lymphocytes [26].
Therefore, we hypothesize that TGFβ1, the IL-7 receptor and IL-7 may add additional objective information to Gleason score and pre-treatment PSA level-based prognosis of prostate cancer-specific survival. In this retrospective study in forty-four patients with localized prostate cancer who underwent radical prostatectomy, we tested this working hypothesis. Prostate cancer-specific survival was examined in relation to the Gleason score, pre-treatment PSA level, age, and prostate tissue expression levels of IL-7, TGFβ1 and the IL-7 receptor.
Materials and methods
Patient samples
Clinical prostate cancer samples (1989–2001) were obtained from the tissue bank of the Erasmus University MC. Samples were snap frozen and stored in liquid nitrogen. All samples contained at least 70% tumor cells. Collection of patient samples was performed according to national legislation concerning ethical requirements. The Erasmus MC Medical Ethics Committee, according to the Medical Research Involving Human Subjects Act, approved the use of these samples. Population characteristics are shown in Table 1, follow-up was completed until December 31, 2008.
RNA isolation and gene expression analysis
RNA from the prostate cancer samples was using RNABee reagent as described by the manufacturer (Tel-test, Inc., Friendswood, TX, USA). The RT reaction was performed with 1 μg RNA from the samples with oligo-(dT)12–18 primer (Invitrogen) and pre-incubated for 10 min at 70°C. First-strand buffer, dithiothreitol, dNTPs and RNAsin were added and incubated for 2 min at 37°C. The RT reaction was initiated by MMLV-RT and incubated for 1 h at 37°C. After this, the reaction was maintained for 10 min at 90°C and immediately thereafter frozen. Quantitative real-time RT-PCR analysis was done with an ABI Prism 7700 Sequence Detection System (Applied Biosystems) using AmpliTaq Gold according to the manufacturer’s specifications (Applied Biosystems, Foster City, CA). The FAM-labeled primers and probes for Taqman Gene Expression Assays were obtained from Applied Biosystems (IL-7, Hs00978525_m1; IL-7receptor, Hs00902334_m1; TGFbeta1, Hs00998133_m1). The CT readings of target gene expressed were normalized to an endogenous reference and relative to a calibrator. The endogenous reference was Porphobilinogen deaminase (PBDG); a mixture of cDNAs of prostate carcinoma xenografts was used as the calibrator [27, 28].
Statistics
With death from prostate cancer as event, and death from other causes considered as censored events, log-rank tests and Cox regressions were performed using base 2 log-transformed pre-treatment PSA levels, and base 2 log-transformed IL-7, IL-7receptor and TGFβ1 relative expression levels. Post-surgical information such as pTNM staging was omitted in this study because of our interest in a possible stronger pre-surgical prognosis, at present mainly based upon the pre-treatment PSA levels and the Gleason score. The relation of the variables on prostate cancer survival was determined, along with Akaike’s information criterion (AIC 2 X ) for the comparison of the models. The AIC 2 X measures the improvement in prognostic value of a model with respect to a model with a sole constant as a predictor (=null-model). Therefore, if two models are compared (using the same underlying dataset), the model with the highest AIC 2 X is to be preferred. Please note that AIC is different than the mentioned AIC 2 X . AIC is defined as the −2log likelihood of the observed data at hand under the assumed model, corrected for the number of degrees of freedom. It refers to the quality of the fit. A perfect fit yields a −2log likelihood of zero, a less than perfect fit a value greater than zero, and therefore the smaller the AIC the better the fit.
Results
Patient characteristics
Forty-four prostate cancer patients were studied, 7 patients died of prostate cancer. All patients underwent radical prostatectomy and had clinical findings reviewed. Patient characteristics and relative cytokine expression levels are reported in Table 1. The median age at diagnosis was 61 years with an interquartile range (IQR) of 9.5 years. The median PSA level pre-treatment was 10.8 ng/ml (IQR: 13.8 ng/ml), and the median Gleason score was 6. Median cytokine levels in the examined prostate cancer tissue samples were 6.0 (IQR: 6.0), 3.4 × 107 (IQR 7.2 × 107) and 44.5 (IQR 48.5) for IL-7, IL-7receptor and TGFβ1, respectively. The median follow-up time was 11.8 years (IQR 5.3 years) after radical prostatectomy.
Analysis of prostate cancer-specific survival
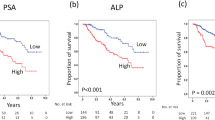
First a log-rank test was performed using the individual variables in relation with prostate cancer-specific survival. Both the Gleason score (P = 0.00) and pre-treatment PSA levels (P = 0.00) did show a relation with prostrate cancer-specific survival, as well as IL-7 receptor (P = 0.00), IL-7 (P = 0.04) and TGFβ1 (P = 0.00). Age at diagnosis (P = 0.91) did not indicate to be related to prostate cancer death. Contribution of separate variables to prostate cancer-specific survival is summarized in Table 2.
Secondly, multivariate analysis with regard to prostate cancer-specific survival was performed (Table 3). The basic model included the Gleason score (hazard ratio (HR) 2.4, confidence interval (CI) 1.0–6.1) and PSA levels pre-treatment (HR 1.4 CI 0.8–2.2), since these two parameters are, among others, used for decision-making on prostate cancer treatment. This basic model was extended using the other variables. Extending the basic model with basic model with the variables IL-7receptor (HR 0.52 CI 0.22–1.20) or age (HR 0.96 CI 0.85–1.09) did not improve the prediction of disease specific survival. The best model for prediction of disease-specific survival included the log-transformed pre-treatment PSA levels (HR 1.6 CI 0.8–3.0), log-transformed TGFβ1 expression (HR 10.4 CI 2.1–52.0), log-transformed IL-7 expression (HR 0.1 CI 0.0–0.9) and the Gleason score (HR 4.2 CI 1.0–17.7). The AIC 2 X were 6.5 and 18.1 for the basic model and the final model, respectively.
Discussion
We analyzed the data of forty-four prostate cancer patients for prostate cancer-specific survival in relation with the Gleason score, PSA-level pre-treatment, age at diagnosis, and the expression levels of IL-7, TGFβ1 and the IL-7 receptor within prostate cancer tissue samples.
Besides the Gleason scores and pre-treatment PSA levels, also the IL-7 receptor, IL-7 and TGFβ1 were related to prostate cancer-specific survival (log-rank test, Table 2). The relation of the Gleason score and PSA levels with prostate cancer prognosis has been reported since the 1960s [3, 29]. Elevated levels of TGFβ1 are associated earlier to be involved in the development of prostate cancer in animal models and accumulation of TGFβ1 in primary and metastatic prostate cancer tissue samples [15–18]. Pre-treatment biomarker levels of for example vascular endothelial growth factor, IL-6 but also TGFβ1 have been indicated to improve the accuracy of post-prostatectomy for prediction of biochemical recurrence, when incorporated into standard predictive models. It was suggested that this incorporation might allow more accurate identification of patients who are likely to fail RP thereby allowing more efficient delivery of adjuvant therapy [30, 31]. It has however also been reported that plasma TGFβ1 was not elevated in prostate cancer patients compared to non-prostate cancer patients. Plasma TGFβ1 levels did not correspond to Gleason score or PSA levels in these patients; however, urinary TGFβ1 levels did [32]. On the other hand, one should take into account that urinary markers might reflect a renal process rather than a prostate cancer process, as well as the variation of serum markers due to underlying disease or age [33–35]. Even though it is difficult to compare these studies because different methods were used in collection and preparation of patient samples, more objective TGFβ1 detection in plasma or other cytokines related to prostate cancer could ease in determination of the prostate cancer process and treatment. Decreased IL-7receptor expression has not been reported before in relation with prostate cancer tissue. However, reduced numbers of IL-7 receptor expressing immune cells and IL-7-signaling defects in peripheral blood were observed in patients with breast cancer [36]. Epithelial IL-7 production was reported to support intraprostatic lymphocyte survival. Its loss in prostate cancer is associated with a severe depletion of prostate-associated lymphocytes and points to a tumor escape mechanism [26].
Functional cytokines are classified in pro-inflammatory (Th1) and anti-inflammatory (Th2). It has been reported that high levels of the anti-inflammatory cytokines IL-4 and IL-10 are associated with elevated levels of PSA [13]. IL-6 is an interleukin that acts as both a pro-inflammatory and anti-inflammatory cytokine. In relation to prostate cancer, elevated levels of IL-6 have been associated with elevated levels of PSA and disease activity [12, 13]. TGFβ1 also belongs to the anti-inflammatory cytokines, and in relation with prostate cancer, elevated levels of TGFβ1 were correlated to disease progression [14–18], which is also observed in our presented model. IL-7, on the other hand, is a pro-inflammatory cytokine. In our model, low levels of IL-7 are associated with poor prostate cancer survival, which reflects the suggested antagonistic relationship between TGFβ and IL-7 [19, 20]. The overall picture for prostate cancer suggests that elevation of anti-inflammatory cytokines is related to poor prostate cancer prognosis, while elevation of pro-inflammatory cytokines reduces the risk [37, 38].
Multivariate models based on the Gleason score and pre-treatment PSA levels extended with other variables have been validated in this study. The final model for prediction of prostate cancer-specific survival included the Gleason score, pre-treatment PSA levels, TGFβ1 expression and IL-7 expression. When Cox regression was performed, hazard ratios, together with their confidence intervals, were presented (P-values lower or equal to 0.05 were considered statistically significant), along with Akaike’s information criterion (AIC 2 X ). A model with base 2 log-transformed variables showed better fitting (observed-expected) compared to non-log-transformed variables (AIC 2 X : 18.05 and 15.89, respectively).
The additional value of TGFβ1 and IL-7 with respect to predicting the natural course of disease was evident, since the prognostic value of the model was almost three times higher than a model including only Gleason score and pre-treatment PSA (AIC 2 X 18.1 vs. AIC 2 X 6.5, respectively). This model also reflects the suggested antagonistic behavior of TGFβ1 and IL-7. High levels of TGFβ1 corresponded with a higher risk, and high IL-7 levels with reduced risk of prostate cancer death. Given the limitations of Gleason grading, the final model was analyzed without the Gleason score (data not shown). This model showed to be less predictive for prostate cancer survival, and the AIC 2 X was lower (AIC 13.5) compared to the final model including the Gleason score (AIC 18.1). Therefore, it was concluded that the predictive value of Gleason score, despite its limitations, could not be omitted in a predictive model for prostate cancer survival.
Given the limited number of patients in this study, these results need to be externally validated in studies with larger prostate cancer patient populations [39]. Nevertheless, our results indicate that IL-7 and TGFβ1 are promising markers to indicate those patients at risk for poor survival. Objectively measured TGFβ1 and IL-7 expression levels in prostate cancer tissues can be of additional value with respect to the biological aggressiveness of the diagnosed prostate cancer and the considered therapy, when incorporated into a predication model containing the Gleason score and pre-treatment PSA levels. If pre-surgical TGFβ1 and IL-7 expression levels could be measured in serum or urine [32], with the same predictive properties as TGFβ1 and IL-7 derived from prostate cancer tissue, the application of the former is likely to be preferred.
References
Eckersberger E, Finkelstein J, Sadri H, Margreiter M, Taneja SS, Lepor H, Djavan B (2009) Screening for prostate cancer: A review of the ERSPC and PLCO trials. Rev Urol 11:127–133
Schroder FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S, Nelen V, Kwiatkowski M, Lujan M, Lilja H, Zappa M, Denis LJ, Recker F, Berenguer A, Maattanen L, Bangma CH, Aus G, Villers A, Rebillard X, van der Kwast T, Blijenberg BG, Moss SM, de Koning HJ, Auvinen A (2009) Screening and prostate-cancer mortality in a randomized European study. N Engl J Med 360:1320–1328
Gleason DF (1966) Classification of prostatic carcinomas. Cancer Chemother Rep 50:125–128
Pinthus JH, Witkos M, Fleshner NE, Sweet J, Evans A, Jewett MA, Krahn M, Alibhai S, Trachtenberg J (2006) Prostate cancers scored as Gleason 6 on prostate biopsy are frequently Gleason 7 tumors at radical prostatectomy: implication on outcome. J Urol 176:979–984; discussion 984
Rajinikanth A, Manoharan M, Soloway CT, Civantos FJ, Soloway MS (2008) Trends in Gleason score: concordance between biopsy and prostatectomy over 15 years. Urology 72:177–182
Allam CK, Bostwick DG, Hayes JA, Upton MP, Wade GG, Domanowski GF, Klein MA, Boling EA, Stilmant MM (1996) Interobserver variability in the diagnosis of high-grade prostatic intraepithelial neoplasia and adenocarcinoma. Mod Pathol 9:742–751
Descazeaud A, Rubin MA, Allory Y, Burchardt M, Salomon L, Chopin D, Abbou C, de la Taille A (2005) What information are urologists extracting from prostate needle biopsy reports and what do they need for clinical management of prostate cancer? Eur Urol 48:911–915
Tsivian M, Sun L, Mouraviev V, Madden JF, Mayes JM, Moul JW, Polascik TJ (2009) Changes in Gleason score grading and their effect in predicting outcome after radical prostatectomy. Urology 74:1090–1093
Orozco R, O’Dowd G, Kunnel B, Miller MC, Veltri RW (1998) Observations on pathology trends in 62, 537 prostate biopsies obtained from urology private practices in the United States. Urology 51:186–195
Muntener M, Epstein JI, Hernandez DJ, Gonzalgo ML, Mangold L, Humphreys E, Walsh PC, Partin AW, Nielsen ME (2008) Prognostic significance of Gleason score discrepancies between needle biopsy and radical prostatectomy. Eur Urol 53:767–775; discussion 775-766
Boorjian SA, Karnes RJ, Crispen PL, Rangel LJ, Bergstralh EJ, Sebo TJ, Blute ML (2009) The impact of discordance between biopsy and pathological Gleason scores on survival after radical prostatectomy. J Urol 181:95–104; discussion 104
Twillie DA, Eisenberger MA, Carducci MA, Hseih WS, Kim WY, Simons JW (1995) Interleukin-6: a candidate mediator of human prostate cancer morbidity. Urology 45:542–549
Wise GJ, Marella VK, Talluri G, Shirazian D (2000) Cytokine variations in patients with hormone treated prostate cancer. J Urol 164:722–725
Adler HL, McCurdy MA, Kattan MW, Timme TL, Scardino PT, Thompson TC (1999) Elevated levels of circulating interleukin-6 and transforming growth factor-beta1 in patients with metastatic prostatic carcinoma. J Urol 161:182–187
Thompson TC, Truong LD, Timme TL, Kadmon D, McCune BK, Flanders KC, Scardino PT, Park SH (1992) Transforming growth factor beta 1 as a biomarker for prostate cancer. J Cell Biochem Suppl 16H:54–61
Truong LD, Kadmon D, McCune BK, Flanders KC, Scardino PT, Thompson TC (1993) Association of transforming growth factor-beta 1 with prostate cancer: an immunohistochemical study. Hum Pathol 24:4–9
Eastham JA, Truong LD, Rogers E, Kattan M, Flanders KC, Scardino PT, Thompson TC (1995) Transforming growth factor-beta 1: comparative immunohistochemical localization in human primary and metastatic prostate cancer. Lab Invest 73:628–635
Perry KT, Anthony CT, Steiner MS (1997) Immunohistochemical localization of TGF beta 1, TGF beta 2, and TGF beta 3 in normal and malignant human prostate. Prostate 33:133–140
Tang J, Nuccie BL, Ritterman I, Liesveld JL, Abboud CN, Ryan DH (1997) TGF-beta down-regulates stromal IL-7 secretion and inhibits proliferation of human B cell precursors. J Immunol 159:117–125
Dubinett SM, Huang M, Dhanani S, Economou JS, Wang J, Lee P, Sharma S, Dougherty GJ, McBride WH (1995) Down-regulation of murine fibrosarcoma transforming growth factor-beta 1 expression by interleukin 7. J Natl Cancer Inst 87:593–597
Blobe GC, Schiemann WP, Lodish HF (2000) Role of transforming growth factor beta in human disease. N Engl J Med 342:1350–1358
Jicha DL, Mule JJ, Rosenberg SA (1991) Interleukin 7 generates antitumor cytotoxic T lymphocytes against murine sarcomas with efficacy in cellular adoptive immunotherapy. J Exp Med 174:1511–1515
Naume B, Espevik T (1991) Effects of IL-7 and IL-2 on highly enriched CD56+ natural killer cells. A comparative study. J Immunol 147:2208–2214
Andersson A, Yang SC, Huang M, Zhu L, Kar UK, Batra RK, Elashoff D, Strieter RM, Dubinett SM, Sharma S (2009) IL-7 promotes CXCR3 ligand-dependent T cell antitumor reactivity in lung cancer. J Immunol 182:6951–6958
Schroten-Loef C, de Ridder CM, Reneman S, Crezee M, Dalgleish A, Todryk SM, Bangma CH, Kraaij R (2009) A prostate cancer vaccine comprising whole cells secreting IL-7, effective against subcutaneous challenge, requires local GM-CSF for intra-prostatic efficacy. Cancer Immunol Immunother 58:373–381
Di Carlo E, D’Antuono T, Pompa P, Giuliani R, Rosini S, Stuppia L, Musiani P, Sorrentino C (2009) The lack of epithelial interleukin-7 and BAFF/BLyS gene expression in prostate cancer as a possible mechanism of tumor escape from immunosurveillance. Clin Cancer Res 15:2979–2987
Hendriksen PJ, Dits NF, Kokame K, Veldhoven A, van Weerden WM, Bangma CH, Trapman J, Jenster G (2006) Evolution of the androgen receptor pathway during progression of prostate cancer. Cancer Res 66:5012–5020
van der Heul-Nieuwenhuijsen L, Dits NF, Jenster G (2009) Gene expression of forkhead transcription factors in the normal and diseased human prostate. BJU Int 103:1574–1580
Rao AR, Motiwala HG, Karim OM (2008) The discovery of prostate-specific antigen. BJU Int 101:5–10
Shariat SF, Walz J, Roehrborn CG, Zlotta AR, Perrotte P, Suardi N, Saad F, Karakiewicz PI (2008) External validation of a biomarker-based preoperative nomogram predicts biochemical recurrence after radical prostatectomy. J Clin Oncol 26:1526–1531
Svatek RS, Jeldres C, Karakiewicz PI, Suardi N, Walz J, Roehrborn CG, Montorsi F, Slawin KM, Shariat SF (2009) Pre-treatment biomarker levels improve the accuracy of post-prostatectomy nomogram for prediction of biochemical recurrence. Prostate 69:886–894
Perry KT, Anthony CT, Case T, Steiner MS (1997) Transforming growth factor beta as a clinical biomarker for prostate cancer. Urology 49:151–155
Mitropoulos D, Kiroudi A, Christelli E, Serafetinidis E, Zervas A, Anastasiou I, Dimopoulos C (2004) Expression of transforming growth factor beta in renal cell carcinoma and matched non-involved renal tissue. Urol Res 32:317–322
Lin Y, Nakachi K, Ito Y, Kikuchi S, Tamakoshi A, Yagyu K, Watanabe Y, Inaba Y, Kazuo T (2009) Variations in serum transforming growth factor-beta1 levels with gender, age and lifestyle factors of healthy Japanese adults. Dis Markers 27:23–28
Porreca E, Di Febbo C, Vitacolonna E, Baccante G, Di Castelnuovo A, Angelini A, Febo F, Di Nisio M, Cuccurullo F (2002) Transforming growth factor-beta1 levels in hypertensive patients: association with body mass index and leptin. Am J Hypertens 15:759–765
Vudattu NK, Magalhaes I, Schmidt M, Seyfert-Margolis V, Maeurer MJ (2007) Reduced numbers of IL-7 receptor (CD127) expressing immune cells and IL-7-signaling defects in peripheral blood from patients with breast cancer. Int J Cancer 121:1512–1519
Hull GW, McCurdy MA, Nasu Y, Bangma CH, Yang G, Shimura S, Lee HM, Wang J, Albani J, Ebara S, Sato T, Timme TL, Thompson TC (2000) Prostate cancer gene therapy: comparison of adenovirus-mediated expression of interleukin 12 with interleukin 12 plus B7–1 for in situ gene therapy and gene-modified, cell-based vaccines. Clin Cancer Res 6:4101–4109
Selleck WA, Canfield SE, Hassen WA, Meseck M, Kuzmin AI, Eisensmith RC, Chen SH, Hall SJ (2003) IFN-gamma sensitization of prostate cancer cells to Fas-mediated death: a gene therapy approach. Mol Ther 7:185–192
Steyerberg EW (2009) Clinical prediction models: a practical approach to development, validation, and updating. Springer, New York
Acknowledgments
The authors thank Dr. R.A. Willemsen, Prof. T.H. van der Kwast, G. Jenster and Prof. S.M. Todryk for their critical reading and feedback.
Conflict of interest
The authors declare that they have no conflict of interest.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Schroten, C., Dits, N.F., Steyerberg, E.W. et al. The additional value of TGFβ1 and IL-7 to predict the course of prostate cancer progression. Cancer Immunol Immunother 61, 905–910 (2012). https://doi.org/10.1007/s00262-011-1159-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00262-011-1159-3