
Abstract
Purpose
To examine the results of segmental transcatheter arterial chemoembolization with doxorubicin-loaded DC Bead in the treatment of hepatocellular carcinoma (HCC) in non-surgical candidates.
Material and methods
Seventy-one patients (60% men; 11% women; mean age 63; range 46–71 years) with documented HCC of 3–10 cm in diameter (mean 6.2) were enrolled prospectively in the study. All patients had cirrhosis-related HCC that was developed on an underlying controlled hepatitis infection. Only patients with compensated cirrhosis—Child A or B—were included in this study.
Results
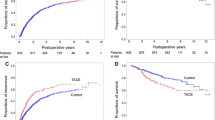
Overall complete response (CR) according to EASL on an intention to treat basis was seen in 11 patients who developed complete necrosis (15.5%). Objective response (OR) ranged from 66.2% to 85.5% across the four treatments. Survival at 12 months was 97.05%. Sustained CR was observed in 11 (16.1%), and OR in 49 (72%). Sustained partial response was seen in 49 patients (72.05%). Survival at 18 months was 94.1%. At 24 months follow-up survival was 91.1%. Sustained OR was seen in 45 patients (66.2%) while sustained CR was 16.1% (11/68). At 30 months survival was 88.2%. One patient with CR developed multifocal HCC in areas that most likely were not embolized during the previous embolization sessions. In this patient recurrence-free survival was 28 months. Alpha Fetroprotein levels decreased significantly in measurements 1 month post each procedure (p < 0.001). Bilirubin, γ-GT, aspartate aminotransferase, alanine aminotransferase, and alkaline phosphatase (ALP) showed only transient increases observed during the study period. Severe procedure-related complications were seen in 4.2% (cholecystitis: n = 1; liver abscess: n = 1; pleural effusion: n = 1). Post Embolization Syndrome (PES) was observed in all patients.
Conclusion
Transcatheter arterial chemoembolization with DC Bead is an effective and safe procedure in the treatment of HCC patients not eligible for curative treatments with high rates of response and high rates of mid term survival.


Similar content being viewed by others

References
Lewis AL, Gonzalez MV, Lloyd AW, et al. (2006) DC bead: in vitro characterization of a drug-delivery device for transarterial chemoembolization. J Vasc Interv Radiol 17:335–342
Hong K, Khwaja A, Liapi E, et al. (2006) New intra-arterial drug delivery system for the treatment of liver cancer: preclinical assessment in a rabbit model of liver cancer. Clin Cancer Res 12:2563–2567
Varela M, Real MI, Burrel M, et al. (2007) Chemoembolization of hepatocellular carcinoma with drug eluting beads: efficacy and doxorubicin pharmacokinetics. J Hepatol 46(3):474–481
Lewis AL, Taylor RR, Hall B, et al. (2006) Pharmacokinetic and safety study of doxorubicin-eluting beads in a porcine model of hepatic arterial embolization. J Vasc Interv Radiol 17(8):1335–1343
Chevret S, Trinchet JC, Mathieu D, et al. (1999) A new prognostic classification for predicting survival in patients with hepatocellular carcinoma. Groupe d’Etude et de Traitement du Carcinome Hepatocellulaire. J Hepatol 31:133–141
Brown DB, Fundakowski CE, Lisker-Melman M (2004) Comparison of MELD and Child-Pugh scores to predict survival after chemoembolization for hepatocellular carcinoma. J Vasc Interv Radiol 15:1209–1218
Bruix J, Sherman M, Llovet JM, et al. (2001) Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona–2000 EASL Conference. European Association for the Study of the Liver. J Hepatol 35:421–430
Padhani AR, Ollivier L (2001) The RECIST criteria: implications for diagnostic radiologists. Br J Radiol 74:983–986
Llovet JM, Real MI, Montana X, et al. (2002) Barcelona Liver Cancer Group. Arterial embolization or chemoembolization versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomized controlled trial. Lancet 359: 1734–1739
Lo CM, Ngan H, Tso WK, et al. (2002) Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology 35:1164–1171
Llovet JM, Bruix J (2003) Systematic review of randomized trials for unresectable hepatocellular carcinoma: chemoembolization improves survival. Hepatology 37:429–442
Pelletier G, Ducreux M, Gay F, et al. (1998) Treatment of unresectable hepatocellular carcinoma with lipiodol chemoembolization: a multicenter randomized trial. J Hepatol 29:129–134
Bruix J, Llovet JM, Castells A, et al. (1999) Transarterial embolization versus symptomatic treatment in patients with advanced hepatocellular carcinoma: results of a randomized, controlled trial in a single institution. Hepatology 27:1578–1583
Matsui O, Kadoya M, Yoshikawa J, et al. (1993) Small hepatocellular carcinoma: treatment with subsegmental transcatheter arterial embolization. Radiology 188:79–83
Saccheri S, Andrea Lovaria A, Sangiovanni A, et al. (2002) Segmental transcatheter arterial chemoembolization treatment in patients with cirrhosis and inoperable hepatocellular carcinomas J Vasc Interv Radiol 13:995–999
Ramsey DE, Kernagis LY, Soulen MC, et al. (2002) Chemoembolization of hepatocellular carcinoma. J Vasc Interv Radiol 13(suppl):S211–S221
Li X, Feng GS, Zheng CS, et al. (2004) Expression of plasma vascular endothelial growth factor in patients with hepatocellular carcinoma and effect of transcatheter arterial chemoembolization therapy on plasma vascular endothelial growth factor level. World J Gastroenterol 10:2878–2882
Gonzalez MV, Lloyd AW, Phillips GJ, et al. (2004) Drug-eluting beads for embolotherapy: drug loading, distribution and release studies. Presented at the 3rd UKSB Meeting (8–9 July 2004), Brighton, UK. Abstract p19
Raoul JL, Heresbach D, Bretagne JF (1992) Chemoembolization of hepatocellular carcinomas. A study of the biodistribution and pharmacokinetics of doxorubicin. Cancer 70(3):585–590
Müller HJ, Port RE, Grubert M, et al. (2003) The influence of liver metastases on the pharmacokinetics of doxorubicin—a population-based pharmacokinetic project of the CESAR-APOH. Int J Clin Pharmacol Ther 41:598–599
Nakashima Y, Nakashima O, Hsia CC, et al. (1999) Vascularization of small hepatocellular carcinoma: correlation with differentiation. Liver 19:12–18
Groupe d’Étude et de Traitment du Carcinome Hépatocellulaire (1995) A comparison of lipiodol chemoembolization and conservative treatment for unresectable hepatocellular carcinoma. N Engl J Med 332:1256–1261
Takayasu K, Muramatsu Y, Maeda T, et al. (2001) Targeted transarterial oily chemoembolization for small hepatocellular carcinoma using a unified helical CT and angiography system. Am J Radiol 176:681–688
Liem MSL, Poon RTP, Lo CM, et al. (2005) Outcome of transarterial chemoembolization in patients with inoperable hepatocellular carcinoma eligible for radiofrequency ablation. World J Gastroenterol 711(29):4465–4471
Wigmore SJ, Redhead DN, Thomson BN, et al. (2003) Postchemoembolization syndrome: tumor necrosis or hepatocyte injury? Br J Cancer 89:1423–1427
Brown DB, Geschwind JF, Soulen MC, et al. (2006) Society of interventional radiology position statement on chemoembolization of hepatic malignancies. J Vasc Interv Radiol 17:217–230
Song S-Y, Chung WJ, Han JK, et al. (2001) Liver abscess after transcatheter oily chemoembolization for hepatic tumors: incidence, predisposing factors, and clinical outcome. J Vasc Interv Radiol 12(3):313–320
Geschwind FH, Kaushik S, Ramsey DE, et al. (2002) Influence of a new prophylactic antibiotic therapy on the incidence of liver abscesses after chemoembolization treatment of liver tumors. J Vasc Interv Radiol 13(11):1163–1166
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Malagari, K., Alexopoulou, E., Chatzimichail, K. et al. Transcatheter chemoembolization in the treatment of HCC in patients not eligible for curative treatments: midterm results of doxorubicin-loaded DC bead. Abdom Imaging 33, 512–519 (2008). https://doi.org/10.1007/s00261-007-9334-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-007-9334-x