
Abstract
Background
CT could be used to evaluate abnormalities in the bowel wall, mesentery, adjacent structures, vasculature, and even the activity of Crohn disease (CD). To our knowledge, few direct comparisons of CD characterization using multidetector row CT with dynamic contrast enhancement, 3D imaging, CT angiography (CTA), and CT-enteroclysis (CT-E) on the same cohort of patients. The purpose of this study was to evaluate the diagnostic value of CD using multidetector helical CT with CT-E, dynamic contrast enhancement, 3D imaging, and CTA.
Methods
Twenty-eight patients known or suspected CD underwent CT-E, dynamic contract enhancement, CTA, and 3D imaging. The multidetector CT series images were performed on eight-slice CT scanner. All the examinations were performed when water was used as an oral contrast starting 25 s after 140 mL of intravenous contrast agent was administered, followed by portal venous phase (60 s), and a 60–70 s delay, then sending 1.25-mm slices to the 3D workstation, CT angiograms and 3D images were reconstructed. All the images were reviewed to detect abnormalities of CD. The abnormalities of the bowel wall, mucosal and submucosal ulceration, prominent perienteric vasculature, sinus tracts or fistulae, abscess were evaluated.
Results
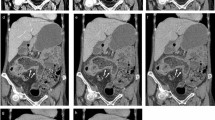
Crohn disease was diagnosed in 28 patients by CT images, and 54 inflammatory segments were revealed. In active inflammatory cases, the diseased bowel wall thickened and the enhancement of diseased bowel wall increased significantly in 34 inflammatory segments of 22 cases, the enhancement of diseased bowel wall increased significantly but without the wall thickened in three patients. Prominent vasculature was found in CTA and 3D images in 21 patients with active diseases. In 16 patients, the sharp interface between bowel and mesentery was lost and the attenuation of fat increased. Sinus tracts or fistulae were observed in eight patients, four of 28 patients demonstrated abscesses, all were active inflammatory patients. In three chronic inflammatory patients, normal bowel, bowel lumen stricture, and the normal enhancement of the wall were displayed.
Conclusion
The abnormalities of CD and its complications can be identified by multidetector CT with CT-E, dynamic enhancement, CTA, and 3D imaging, and they are important methods in diagnosing CD. Complications of CD can be shown better when CT-E is performed.



Similar content being viewed by others


Abbreviations
- CD:
-
Crohn disease
- CT-E:
-
CT enteroclysis
- CTA:
-
CT angiography
References
Loftus EV Jr, Schoenfeld P, Sandborn WJ (2002) The epidemiology and natural history of Crohn disease in population-based patient cohorts from North America: a systematic review. Aliment Pharmacol Ther 16:51–60
Doerfler OC, Ruppert-Kohlmayr AJ, Reittner P, et al. (2003) Helical CT of the small bowel with an alternative oral contrast material in patients with Crohn disease. Abdom Imaging 28(3):313–318
Rollandi GA, Curone PF, Biscaldi E, et al. (1999) Spiral CT of the abdomen after distention of small bowel loops with transparent enema in patients with Crohn’s disease. Abdom Imaging 24:544–549
Boudiaf M, Jaff A, Soyer P, et al. (2004) Small-bowel disease: prospective evaluation of multi-detector row helical CT enteroclysis in 107 consecutive patients. Radiology 233:338–344
Campo LD, Arribas I, Valbuena M, et al. (2001) Spiral CT findings in active and remission phases in patients with Crohn disease. J Comput Assist Tomogr 25:792–797
Meyers MA, McGuire PV (1995) Spiral CT demonstration of hypervascularity in Crohn’s disease: vascular jejunization of the ileum or the comb sign. Abdom Imaging 20:327–332
Lee SS, Ha HK, Yang SK, et al. (2002) CT of prominent pericolic or perienteric vasculature in patients with Crohn’s disease: correlation with clinical disease activity and findings on barium studies. AJR 179:1029–1036
Gore RM, Balthazar EJ, Ghahremani GG, et al. (1996) CT features of ulcerative colitis and Crohn’s disease. AJR 167:3–15
Turetschek K, Schober E, Wunderbaldinger P, et al. (2002) Findings at helical CT-enteroclysis in symptomatic patients with Crohn disease: correlation with endoscopic and surgical findings. J Comput Assist Tomogr 26:488–492
Gossios KJ, Tsianos EV (1997) Crohn disease: CT findings after treatment. Abdom Imaging 22:160–163
Wold PB, Fletcher JG, Johnson CD, et al. (2003) Assessment of small bowel Crohn disease: noninvasive peroral CT enterography compared with other imaging methods and endoscopy-feasibility study. Radiology 229:275–281
Zissin R, Gayer G, Kots E, et al. (2001) Iliopsoas abscess: a report of 24 patients diagnosed by CT. Abdom Imaging 26:533–539
Zissin R, Hertz M, Paran H, et al. (2004) Small bowel obstruction secondary to Crohn disease: CT findings. Abdom Imaging 2:320–325
Maniatis V, Chryssikopoulos H, Roussakis A, et al. (2000) Perforation of the alimentary tract: evaluation with computed tomography. Abdom Imaging 25:373–379
Jabra AA, Fishman EK (1997) Small bowel obstruction in the pediatric patient: CT evaluation. Abdom Imaging 22:466–470
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Liu, Y.B., Liang, C.H., Zhang, Z.L. et al. Crohn disease of small bowel: multidetector row CT with CT enteroclysis, dynamic contrast enhancement, CT angiography, and 3D imaging. Abdom Imaging 31, 668–674 (2006). https://doi.org/10.1007/s00261-006-9092-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-006-9092-1