
Abstract
Purpose
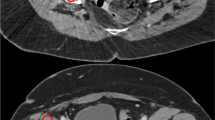
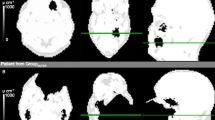
In combined whole-body PET/MR, attenuation correction (AC) is performed indirectly using the available MR image information and subsequent segmentation. Implant-induced susceptibility artifacts and subsequent signal voids may challenge MR-based AC (MR-AC). We evaluated the accuracy of MR-AC in PET/MR in patients with metallic endoprostheses, and propose a clinically feasible correction method.
Methods
We selected patients with uni- or bilateral endoprostheses from 61 consecutive referrals for whole-body PET/MR imaging (mMR; Siemens Healthcare). Simultaneous whole-body PET/MR imaging was performed at 120 min after injection of about 300 MBq [18F]FDG. MR-AC was performed using (1) original MR images and subsequent Dixon water–fat segmentation, (2) as method 1 with implant-induced signal voids filled with soft tissue, (3) as method 2 with superimposed coregistered endoprostheses from the CT scan, and (4) as method 1 with implant-induced signal voids filled with metal. Following MR-AC (methods 1–4) PET emission images were reconstructed on 344 × 344 matrices using attenuation-weighted OSEM (three iterations, 21 subsets, 4 mm gaussian). Maximum body-weight normalized standardized uptake values (SUVmax) were obtained for both hips. Mean SUV (SUVmean) in homogeneous reference regions in the gluteal muscle and bladder following MR-AC (methods 1–4) are also reported.
Results
In total, four patients presented with endoprostheses, unilateral in two and bilateral in two. The fraction of voxels in MR images affected by the implant was at least twice that of the voxels representing the actual implants. MR-AC using methods 2 and 3 recovered the FDG distribution pattern compared to uncorrected PET images and method 1, while method 4 resulted in severe overestimation of FDG uptake (>460 % SUVmax). When compared to method 1, relative changes in SUVmean in the reference regions from method 2 and 3 were generally small albeit not correlated with the fraction of the attenuation image affected by implant-induced artifacts.
Conclusions
Endoprostheses cause PET/MR artifacts that exceed the volume occupied by the implants, and bias PET quantification. Artifacts and bias can be corrected by semiautomated inpainting with soft tissue with a single composition prior to MR-AC, thus restoring quantitative activity distribution.




Similar content being viewed by others

References
Hillner B, Siegel B, Liu D, Shields AF, Gareen IF, Hanna L, et al. Impact of positron emission tomography/computed tomography and positron emission tomography (PET) alone on expected management of patients with cancer: initial results from the National Oncologic PET Registry. J Clin Oncol. 2008;26:2155–61.
Zhuang H, Alavi A. 18-Fluorodeoxyglucose positron emission tomographic imaging in the detection and monitoring of infection and inflammation. Semin Nucl Med. 2002;32:47–59.
Haroon A, Zumla A, Bomanji J. Role of fluorine 18 fluorodeoxyglucose positron emission tomography-computed tomography in focal and generalized infectious and inflammatory disorders. Clin Infect Dis. 2012;54:1333–41.
Mumme T, Reinartz P, Cremerius U, Hermanns B, Müller-Rath R, Neuss M, et al. [F-18]-fluorodeoxyglucose (FDG) positron emission tomography (PET) as a diagnostic for hip endoprosthesis loosening. Z Orthop Ihre Grenzgeb. 2003;141:540–6.
Mayer-Wagner S, Mayer W, Maegerlein S, Linke R, Jansson V, Müller PE. Use of 18F-FDG-PET in the diagnosis of endoprosthetic loosening of knee and hip implants. Arch Orthop Trauma Surg. 2010;130:1231–8.
Beyer T, Freudenberg L, Czernin J, Townsend DW. The future of hybrid imaging – part 3: PET/MR, small animal imaging and beyond. Insights Imaging. 2011;2:235–46.
Beyer T, Freudenberg L, Townsend DW, Czernin J. The future of hybrid imaging – part 1: hybrid imaging technologies and SPECT/CT. Insights Imaging. 2011;2:161–9.
Beyer T, Townsend D, Czernin J, Freudenberg LS. The future of hybrid imaging – part 2: PET/CT. Insights Imaging. 2011;2:225–34.
Wahl RL, Quint LE, Cieslak RD, Aisen AM, Koeppe RA, Meyer CR. “Anatometabolic” tumor imaging: fusion of FDG PET with CT or MRI to localize foci of increased activity. J Nucl Med. 1993;34:1190–7.
Kinahan P, Hasegawa B, Beyer T. X-ray based attenuation correction for PET/CT scanners. Semin Nucl Med. 2003;33:166–79.
Pichler B, Kolb A, Nägele T, Schlemmer HP. PET/MRI: paving the way for the next generation of clinical multimodality imaging applications. J Nucl Med. 2010;51:333–6.
Hofmann M, Pichler B, Schölkopf B, Beyer T. Towards quantitative PET/MRI: a review of MR-based attenuation correction techniques. Eur J Nucl Med Mol Imaging. 2009;36 Suppl 1:S93–104.
Boellaard R, O’Doherty M, Weber WA, Mottaghy FM, Lonsdale MN, Stroobants SG, et al. FDG PET and PET/CT: EANM procedure guidelines for tumour PET imaging: version 1.0. Eur J Nucl Med Mol Imaging. 2010;37:181–200.
Brix G, Lechel U, Glatting G, Ziegler SI, Münzing W, Müller SP, et al. Radiation exposure of patients undergoing whole-body dual-modality 18F-FDG PET/CT examinations. J Nucl Med. 2005;46:608–13.
Cahir J, Toms AP. CT and MRI of hip replacements. Orthop Traumatol. 2009;23:101–8.
Kinahan PE, Townsend DW, Beyer T, Sashin D. Attenuation correction for a combined 3D PET/CT scanner. Med Phys. 1998;25:2046–53.
Kalemis A, Delattre B, Heinzer S. Sequential whole-body PET/MR scanner: concept, clinical use and optimisations after two years in the clinic. The manufacturer’s perspective. MAGMA. 2012. doi:10.1007/s10334-012-0330-y.
Delso G, Fürst S, Jakoby B, Ladebeck R, Ganter C, Nekolla SG, et al. Performance measurements of the Siemens mMR integrated whole-body PET/MR scanner. J Nucl Med. 2011;52:1914–22.
Martinez-Möller A, Souvatzoglou M, Delso G, Bundschuh RA, Chefd'hotel C, Ziegler SI, et al. Tissue classification as a potential approach for attenuation correction in whole-body PET/MRI: evaluation with PET/CT data. J Nucl Med. 2009;50:520–6.
Ramos-Cabrer P, van Duynhoven JP, Van der Toorn A, Nicolay K. MRI of hip prostheses using single-point methods: in vitro studies towards the artifact-free imaging of individuals with metal implants. Magn Reson Imaging. 2004;22:1097–103.
Pauchard Y, Smith MR, Mintchev MP. Improving geometric accuracy in the presence of susceptibility difference artifacts produced by metallic implants in magnetic resonance imaging. IEEE Trans Med Imaging. 2005;24:1387–99.
Reft C, Alecu R, Das IJ, Gerbi BJ, Keall P, Lief E, et al. Dosimetric considerations for patients with HIP prostheses undergoing pelvic irradiation. Report of the AAPM Radiation Therapy Committee Task Group 63. Med Phys. 2003;30:1162–82.
Berger MJ, Hubbell JH, Seltzer SM, Chang J, Coursey JS, Sukumar R, et al. XCOM: Photon cross sections database. NIST, PML, Radiation and Biomolecular Physics Division. 1999. http://www.nist.gov/pml/data/xcom/index.cfm. Accessed 13 Dec 2012.
Joemai RM, de Bruin PW, Veldkamp WJ, Geleijns J. Metal artifact reduction for CT: development, implementation, and clinical comparison of a generic and a scanner-specific technique. Med Phys. 2012;39:1125–32.
Meyer E, Raupach R, Lell M, Schmidt B, Kachelrieß M. Frequency split metal artifact reduction (FSMAR) in computed tomography. Med Phys. 2012;39:1904–16.
Schäfers K, Raupach R, Beyer T. Combined 18F-FDG-PET/CT imaging of the head and neck. An approach to metal artifact correction. Nuklearmedizin. 2006;45:219–22.
Acknowledgment
The PET/MR system was donated by the John and Birthe Meyer Foundation. The XD3 software licence was provided by Mirada Medical, Oxford, UK.
Conflicts of interest
T.B. is founder and employee of cmi-experts GmbH, Zurich, Switzerland, and reports no conflicts of interest with this study or the text of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ladefoged, C.N., Andersen, F.L., Keller, S.H. et al. PET/MR imaging of the pelvis in the presence of endoprostheses: reducing image artifacts and increasing accuracy through inpainting. Eur J Nucl Med Mol Imaging 40, 594–601 (2013). https://doi.org/10.1007/s00259-012-2316-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-012-2316-4