
Abstract
Purpose
The aim of this study was to evaluate the clinical value of FDG PET/CT in patients with suspected ovarian cancer recurrence as compared with diagnostic CT, and to assess the impact of the results of FDG PET/CT on treatment planning.
Methods
Included in this retrospective study were 60 patients with suspected recurrent ovarian cancer who had previously undergone primary debulking surgery and had been treated with adjuvant chemotherapy. Diagnostic CT and FDG PET/CT imaging were performed for all patients as clinically indicated. The changes in the clinical management of patients according to the results of FDG PET/CT were also analysed.
Results
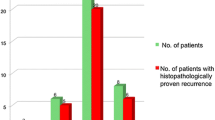
FDG PET/CT was performed in 21 patients with a previously negative or indeterminate diagnostic CT scan, but an elevated CA-125 level, and provided a sensitivity of 95% in the detection of recurrent disease. FDG PET/CT revealed recurrent disease in 19 patients. In 17 of 60 patients, the indication for FDG PET/CT was an elevated CA-125 level and an abnormal diagnostic CT scan to localize accurately the extent of disease. FDG PET/CT scans correctly identified recurrent disease in 16 of the 17 patients, a sensitivity of 94.1%. Moreover, FDG PET/CT was performed in 18 patients with clinical symptoms of ovarian cancer recurrence, an abnormal diagnostic CT scan, but a normal CA-125 level. In this setting, FDG PET/CT correctly confirmed recurrent disease in seven patients providing a sensitivity of 100% in determining recurrence. In four patients, FDG PET/CT was carried out for the assessment of treatment response. Three of four scans were classified as true-negative indicating a complete response. In the other patient, FDG PET/CT identified progression of disease. In total, 45 (75%) of the 60 patients had recurrent disease, in 14 (31.1%) documented by histopathology and in 31 (68.9%) on clinical follow-up, while 15 (25%) had no evidence of recurrent disease. The overall sensitivity, specificity, accuracy, and positive and negative predictive value of FDG PET/CT were significantly superior to those of diagnostic CT (95.5% vs. 55.5%, 93.3% vs. 66.6%, 95% vs. 58.3%, 97.7% vs. 83.3%, 87.7% vs. 33.3%, respectively; p = 0.02) in the detection of recurrent ovarian cancer. FDG PET/CT changed the management in 31 patients (51.6%). It led to the use of previously unplanned treatment procedures in 19 patients (61.2%) and the avoidance of previously planned therapeutic procedures in 12 patients (38.8%).
Conclusion
Our results confirm that FDG PET/CT is a superior posttherapy surveillance modality for the detection of recurrent ovarian cancer than diagnostic CT imaging. Furthermore, integrated FDG PET/CT was useful specifically in optimizing the treatment plan and it might play an important role in treatment stratification in the future.



Similar content being viewed by others

References
Bristow RE, Duska LR, Lambrou NC, Fishman EK, O’Neill MJ, Trimble EL, et al. A model for predicting surgical outcome in patients with advanced ovarian carcinoma using computed tomography. Cancer 2000;89:1532–40.
Cannistra SA. Cancer of the ovary. N Engl J Med 2004;351:2519–29.
Berek JS, Tropé C, Vergote I. Surgery during chemotherapy and at relapse of ovarian cancer. Ann Oncol 1999;10:3–7.
McGuire WP, Hoskins WJ, Brady MF, Kucera PR, Partridge EE, Look KY, et al. Cyclophosphamide and cisplatin compared with paclitaxel and cisplatin in patients with stage III and stage IV ovarian cancer. N Engl J Med 1996;334:1–6.
Pannu HK, Bristow RE, Cohade C, Fishman EK, Wahl RL. PET-CT in recurrent ovarian cancer: initial observations. Radiographics 2004;24:209–23.
Niloff JM, Bast RC Jr, Schaetzl EM, Knapp RC. Predictive value of CA 125 antigen levels in second-look procedures for ovarian cancer. Am J Obstet Gynecol 1985;151:981–6.
Rustin G, Tuxen M. Use of CA 125 in follow-up of ovarian cancer. Lancet 1996;348:191–2.
De Rosa V, Mangoni di Stefano ML, Brunetti A, Caraco C, Graziano R, Gallo MS, et al. Computed tomography and second-look surgery in ovarian cancer patients. Correlation, actual role and limitations of CT scan. Eur J Gynaecol Oncol 1995;16:123–9.
Ferrozzi F, Bova D, De Chiara F, Garlaschi G, Draghi F, Cocconi G, et al. Thin-section CT follow-up of metastatic ovarian carcinoma correlation with levels of CA-125 marker and clinical history. Clin Imaging 1998;22:364–70.
Topuz E, Aydiner A, Saip P, Eralp Y, Taş F, Salihoğlu Y, et al. Correlations of serum CA125 level and computerized tomography (CT) imaging with laparotomic findings following intraperitoneal chemotherapy in patients with ovarian cancer. Eur J Gynaecol Oncol 2000;21:599–602.
Ricke J, Sehouli J, Hach C, Hänninen EL, Lichtenegger W, Felix R. Prospective evaluation of contrast-enhanced MRI in the depiction of peritoneal spread in primary or recurrent ovarian cancer. Eur Radiol 2003;13:943–9.
Prayer L, Kainz C, Kramer J, Stiglbauer R, Schurawitzki H, Baldt M, et al. CT and MR accuracy in the detection of tumor recurrence in patients treated for ovarian cancer. J Comput Assist Tomogr 1993;17:626–32.
Forstner R, Hricak H, Occhipinti KA, Powell CB, Frankel SD, Stern JL. Ovarian cancer: staging with CT and MR imaging. Radiology 1995;197:619–26.
Tempany CM, Zou KH, Silverman SG, Brown DL, Kurtz AB, McNeil BJ. Staging of advanced ovarian cancer: comparison of imaging modalities – report from the Radiological Diagnostic Oncology Group. Radiology 2000;215:761–7.
Schelbert HR, Hoh CK, Royal HD, Brown M, Dahlbom MN, Dehdashti F, et al. Procedure guideline for tumor imaging using fluorine-18-FDG. J Nucl Med 1998;39:1302–5.
Kostakoglu L, Agress H Jr, Goldsmith SJ. Clinical role of FDG PET in evaluation of cancer patients. Radiographics 2003;23:315–40.
Yen TC, Lai CH. Positron emission tomography in gynecologic cancer. Semin Nucl Med 2006;36:93–104.
Zimny M, Siggelkow W, Schröder W, Nowak B, Biemann S, Rath W, et al. 2-[Fluorine-18]-fluoro-2-deoxy-d-glucose positron emission tomography in the diagnosis of recurrent ovarian cancer. Gynecol Oncol 2001;83:310–5.
Rose PG, Faulhaber P, Miraldi F, Abdul-Karim FW. Positive emission tomography for evaluating a complete clinical response in patients with ovarian or peritoneal carcinoma: correlation with second-look laparotomy. Gynecol Oncol 2001;82:17–21.
Chang WC, Hung YC, Kao CH, Yen RF, Shen YY, Lin CC. Usefulness of whole body positron emission tomography (PET) with 18F-fluoro-2-deoxyglucose (FDG) to detect recurrent ovarian cancer based on asymptomatically elevated serum levels of tumor marker. Neoplasma 2002;49:329–33.
Sironi S, Messa C, Mangili G, Zangheri B, Aletti G, Garavaglia E, et al. Integrated FDG PET/CT in patients with persistent ovarian cancer: correlation with histologic findings. Radiology 2004;233:433–40.
Pannu HK, Cohade C, Bristow RE, Fishman EK, Wahl RL. PET-CT detection of abdominal recurrence of ovarian cancer: radiologic-surgical correlation. Abdom Imaging 2004;29:398–403.
Hauth EA, Antoch G, Stattaus J, Kuehl H, Veit P, Bockisch A, et al. Evaluation of integrated whole-body PET/CT in the detection of recurrent ovarian cancer. Eur J Radiol 2005;56:263–8.
Bristow RE, Giuntoli RL 2nd, Pannu HK, Schulick RD, Fishman EK, Wahl RL. Combined PET/CT for detecting recurrent ovarian cancer limited to retroperitoneal lymph nodes. Gynecol Oncol 2005;99:294–300.
Mangili G, Picchio M, Sironi S, Viganò R, Rabaiotti E, Bornaghi D, et al. Integrated PET/CT as a first-line re-staging modality in patients with suspected recurrence of ovarian cancer. Eur J Nucl Med Mol Imaging 2007;34:658–66.
Thrall MM, DeLoia JA, Gallion H, Avril N. Clinical use of combined positron emission tomography and computed tomography (FDG-PET/CT) in recurrent ovarian cancer. Gynecol Oncol 2007;105:17–22.
Chung HH, Kang WJ, Kim JW, Park NH, Song YS, Chung JK, et al. Role of [18F]FDG PET/CT in the assessment of suspected recurrent ovarian cancer: correlation with clinical or histological findings. Eur J Nucl Med Mol Imaging 2007;34:480–6.
Sebastian S, Lee SI, Horowitz NS, Scott JA, Fischman AJ, Simeone JF, et al. PET-CT vs. CT alone in ovarian cancer recurrence. Abdom Imaging 2008;33:112–8.
Hubner KF, McDonald TW, Niethammer JG, Smith GT, Gould HR, Buonocore E. Assessment of primary and metastatic ovarian cancer by positron emission tomography (PET) using 2-[18F]deoxyglucose (2-[18F]FDG). Gynecol Oncol 1993;51:197–204.
Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 2000;92:205–16.
Omura GA, Brady MF, Homesley HD, Yordan E, Major FJ, Buchsbaum HJ, et al. Long-term follow-up and prognostic factor analysis in advanced ovarian carcinoma: the Gynecologic Oncology Group experience. J Clin Oncol 1991;9:1138–50.
Coakley FV, Choi PH, Gougoutas CA, Pothuri B, Venkatraman E, Chi D, et al. Peritoneal metastases: detection with spiral CT in patients with ovarian cancer. Radiology 2002;223:495–9.
AAssar OS, Fischbein NJ, Caputo GR, Kaplan MJ, Price DC, Singer MI, et al. Metastatic head and neck cancer: role and usefulness of FDG PET in locating occult primary tumors. Radiology 1999;210:177–81.
Lowe VJ, Fletcher JW, Gobar L, Lawson M, Kirchner P, Valk P, et al. Prospective investigation of positron emission tomography in lung nodules. J Clin Oncol 1998;16:1075–84.
García-Velloso MJ, Jurado M, Ceamanos C, Aramendía JM, Garrastachu MP, López-García G, et al. Diagnostic accuracy of FDG PET in the follow-up of platinum-sensitive epithelial ovarian carcinoma. Eur J Nucl Med Mol Imaging 2007;34:1396–405.
Antoch G, Saoudi N, Kuehl H, Dahmen G, Mueller SP, Beyer T, et al. Accuracy of whole-body dual-modality fluorine-18-2-fluoro-2-deoxy-D-glucose positron emission tomography and computed tomography (FDG-PET/CT) for tumor staging in solid tumors: comparison with CT and PET. J Clin Oncol 2004;22:4357–68.
Picchio M, Sironi S, Messa C, Mangili G, Landoni C, Gianolli L, et al. Advanced ovarian carcinoma: usefulness of [(18)F]FDG-PET in combination with CT for lesion detection after primary treatment. Q J Nucl Med 2003;47:77–84.
Sironi S, Picchio M, Landoni C, Galimberti S, Signorelli M, Bettinardi V, et al. Post-therapy surveillance of patients with uterine cancers: value of integrated FDG PET/CT in the detection of recurrence. Eur J Nucl Med Mol Imaging 2007;34:472–9.
Iagaru AH, Mittra ES, McDougall IR, Quon A, Gambhir SS. 18F-FDG PET/CT evaluation of patients with ovarian carcinoma. Nucl Med Commun 2008;29:1046–51.
Risum S, Høgdall C, Loft A, Berthelsen AK, Høgdall E, Nedergaard L, et al. The diagnostic value of PET/CT for primary ovarian cancer – a prospective study. Gynecol Oncol 2007;105:145–9.
Nanni C, Rubello D, Farsad M, De Iaco P, Sansovini M, Erba P, et al. (18)F-FDG PET/CT in the evaluation of recurrent ovarian cancer: a prospective study on forty-one patients. Eur J Surg Oncol 2005;31:792–7.
Torizuka T, Nobezawa S, Kanno T, Futatsubashi M, Yoshikawa E, Okada H, et al. Ovarian cancer recurrence: role of whole-body positron emission tomography using 2-[fluorine-18]-fluoro-2-deoxy-D-glucose. Eur J Nucl Med Mol Imaging 2002;29:797–803.
Simcock B, Neesham D, Quinn M, Drummond E, Milner A, Hicks RJ. The impact of PET/CT in the management of recurrent ovarian cancer. Gynecol Oncol 2006;103:271–6.
Fulham MJ, Carter J, Baldey A, Hicks RJ, Ramshaw JE, Gibson M. The impact of PET-CT in suspected recurrent ovarian cancer: a prospective multi-centre study as part of the Australian PET Data Collection Project. Gynecol Oncol 2009;112:462–8.
Avril NE, Weber WA. Monitoring response to treatment in patients utilizing PET. Radiol Clin North Am. 2005;43:189–204.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bilici, A., Ustaalioglu, B.B.O., Seker, M. et al. Clinical value of FDG PET/CT in the diagnosis of suspected recurrent ovarian cancer: is there an impact of FDG PET/CT on patient management?. Eur J Nucl Med Mol Imaging 37, 1259–1269 (2010). https://doi.org/10.1007/s00259-010-1416-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-010-1416-2