
Abstract
Aim
To investigate the variation in biological effective dose (BED) produced by the uncertainty in absorbed dose and radiobiological parameters in Zevalin radioimmunotherapy.
Methods
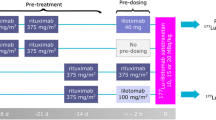
Eight patients scheduled for treatment with standard administration of 90Y-ibritumomab tiuxetan (Zevalin) were studied. Patient-specific pretherapy dosimetry was performed by injection of 111In-ibritumomab tiuxetan. Absorbed doses and BEDs were calculated for critical organs (COs) and tumours, assuming a 30% dose uncertainty and varying the radiobiological parameters in a reasonable range. In an activity-escalation study, BEDs for the COs were compared with the BED limits of external beam radiotherapy (EBRT) and BEDs for the tumour with the EBRT dose prescriptions.
Results
At standard activities, the absorbed doses per unit activity for the COs were in agreement with those in the literature. Absorbed doses to lesions were rather variable, ranging from 1.47 to 16.7 Gy/GBq. Median tumour absorbed dose to lesions in the range 80–110 g was 9.6 Gy/GBq (range 9.2–16.7 Gy/GBq), yielding a mean BED of about 12 Gy for administration of 15 MBq/kg. For the administration of the myeloablative activity of 45 MBq/kg, risk of liver toxicity in one patient would have been foreseen by the model. Considering also the dose uncertainty, the potential risk of liver toxicity in one more patient, lung toxicity in one patient, and kidney toxicity in one patient would have been suggested. The absorbed dose uncertainty was found to be the main source of uncertainty in the BED. As for radiobiological parameters, at myeloablative activities, the increase in the repair half-time for sublethally damaged tissue (Tμ) from 0.5 h to 5 h induced more consistent increases in mean BED/BEDlimit than α/β variation from 2 Gy to 5 Gy: at 53 MBq/kg, 38% for the liver, and 34% for the lungs and kidneys (about threefold higher than that obtained for the increase α/β).
Conclusion
At standard activities, absorbed doses to lesions appear to be effective, even though lower than prescribed by EBRT. At myeloablative dosages, the uncertainty associated with the absorbed doses and radiobiological parameters considerably affect BED evaluation and may account for possible “second-organ” toxicities.








Similar content being viewed by others

References
Wiseman GA, Kornmehl E, Leigh B, Erwin WD, Podoloff DA, Spies S, et al. Radiation dosimetry results and safety correlations from 90Y-ibritumomab tiuxetan radioimmunotherapy for relapsed or refractory non-Hodgkin’s lymphoma: combined data from 4 clinical trials. J Nucl Med 2003;44:465–74.
Wiseman GA, White CA, Sparks RB, et al. Biodistribution and dosimetry results from phase III prospectively randomized, controlled trial of Zevalin™ radioimmunotherapy for low-grade, follicular, or transformed B-cell non-Hodgkin’s lymphoma. Crit Rev Oncol Hematol 2001;39:181–94.
Wiseman GA, White CA, Stabin M, et al. Phase I/II 90Y-Zevalin (yttrium-90 ibritumomab tiuxetan, IDEC-Y2B8) radioimmunotherapy dosimetry results in relapsed or refractory non-Hodgkin’s lymphoma. Eur J Nucl Med 2000;27:766–77.
Cremonesi M, Ferrari M, Grana CM, Vanazzi A, Stabin M, Bartolomei M, et al. High-dose radioimmunotherapy with 90Y-Ibritumomab Tiuxetan: comparative dosimetric study for tailored treatment. J Nucl Med 2007;48:1871–9.
Devizzi L, Guidetti A, Tarella C, Magni M, Matteucci P, Seregni E, et al. High-dose yttrium-90-ibritumomab tiuxetan with tandem stem-cell reinfusion: an outpatient preparative regimen for autologous hematopoietic cell transplantation. J Clin Oncol 2008;26:5175–82.
Chiesa C, Botta F, Coliva A, Maccauro M, Devizzi L, Guidetti A, et al. Absorbed dose and biologically effective dose in patients with high-risk non-Hodgkin’s lymphoma treated with high-activity myeloablative 90Y-ibritumomab tiuxetan (Zevalin). Eur J Nucl Med Mol Imaging 2009;36:1745–57.
Baechler S, Hobbs RF, Prideaux AR, Recordon M, Bischof-Delaloye A, Sgouros G. Estimates of radiation-absorbed dose to kidneys in patients treated with 90Y-ibritumomab tiuxetan. Cancer Biother Radiopharm 2008;23:633–9.
Barone R, Borson-Chazot F, Valkema R, et al. Patient specific dosimetry in predicting renal toxicity with 90YDOTATOC: relevance of kidney volume and dose rate in finding a dose-effect relationship. J Nucl Med 2005;46:99S–106.
Pacilio M, Betti M, Cicone F, et al. Improvement of 90Y-Zevalin dosimetry by indirect Monte Carlo calculation of tumor biologically effective doses and their correlation with clinical outcomes. Preliminary results (abstract). Eur J Nucl Med Mol Imaging 2008;35(Suppl 2):S235.
Howell RW, Murty Goddu S, Rao DV. Application of the linear-quadratic model to radioimmunotherapy: further support for the advantage of longer-lived radionuclides. J Nucl Med 1994;35:1861–69.
Dale RG. The application of the linear-quadratic dose-effect equation to fractionated and protracted radiotherapy. Br J Radiol 1985;58:515–28.
Millar WT. Application of the linear-quadratic model with incomplete repair to radionuclide directed therapy. Br J Radiol 1991;64:242–51.
Brenner DJ, Hlatky LR, Hahnfeldt PJ, Huang Y, Sachs RK. The linear-quadratic model and most other common radiobiological models result in similar predictions of time-dose relationships. Radiat Res 1998;150:83–91.
Baechler S, Hobbs RF, Prideaux AR, et al. Extension of the biological effective dose to the MIRD schema and possible implications in radionuclide therapy dosimetry. Med Phys 2008;35:1123–33.
Emami B, Lyman J, Brown A, Coia L, Goitein M, Munzenrider JE, et al. Tolerance of normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol Phys 1991;21:109–22.
Rachel KB, Evans PM, Flux GD. Application of the linear-quadratic model to combined modality radiotherapy. Int J Radiat Oncol Biol Phys 2004;59:228–41.
Bodey RK, Flux GD, Evans PM. Combining dosimetry for targeted radionuclide and external beam therapies using the biologically effective dose. Cancer Biother Radiopharm 2003;18:89–97.
Stabin MG. Uncertainties in internal dose calculations for radiopharmaceuticals. J Nucl Med 2008;49:853–60.
Cicone F, Baldini R, Cox MC, Russo E, Torelli F, Tofani A, et al. Radioimmunotherapy of heavily pre-treated, non-Hodgkin lymphoma patients: efficacy and safety in a routine setting. Anticancer Res 2009;29:4771–4778.
Tennvall J, Fischer M, Bischof Delaloye A, Bombardieri E, Bodei L, Giammarile F, et al. EANM procedure guideline for radio-immunotherapy for B-cell lymphoma with 90Y-radiolabelled ibritumomab tiuxetan (Zevalin). Eur J Nucl Med Mol Imaging 2007;34:616–22.
Juweid ME, Stroobants S, Hoekstra OS, Mottaghy FM, Dietlein M, Guermazi A, et al; Imaging Subcommittee of International Harmonization Project in Lymphoma. Use of positron emission tomography for response assessment of lymphoma: consensus of the Imaging Subcommittee of International Harmonization Project in Lymphoma. J Clin Oncol 2007;25:571–8.
Erdi YE, Wessels BW, Loew MH, Erdi AK. Threshold estimation in single photon emission computed tomography and planar imaging for clinical radioimmunotherapy. Cancer Res 1995;55:5823s–6.
Stabin MG, Sparks RB, Crowe E. OLINDA/EXM: the second-generation personal computer software for internal dose assessment in nuclear medicine. J Nucl Med 2005;46:1023–7.
Siegel JA, Thomas SR, Stubbs JB, et al. MIRD pamphlet no. 16: Techniques for quantitative radiopharmaceutical biodistribution data acquisition and analysis for use in human radiation dose estimates. J Nucl Med 1999;40:37S–61S.
Buijs WC, Siegel JA, Boerman OC, Corstens FH. Absolute organ activity estimate by five different methods of background correction. J Nucl Med 1998;39:2167–72.
Sgouros G. Bone marrow dosimetry for radioimmunotherapy: theoretical considerations. J Nucl Med 1993;34:689–94.
Wessels BW, Bolch WE, Bouchet LG, Breitz HD, DeNardo GL, Meredith RF, et al. Bone marrow dosimetry using blood-based models for radiolabeled antibody therapy: a multiinstitutional comparison. J Nucl Med 2004;45:1725–33.
Chiesa C, Botta F, Di Betta E, Coliva A, Maccauro M, Aliberti G, et al. Dosimetry in myeloablative 90Y-labeled ibritumomab tiuxetan therapy: possibility of increasing administered activity on the base of biological effective dose evaluation. Preliminary results. Cancer Biother Radiopharm 2007;22:113–20.
Bolch WE, Bouchet LG, Robertson JS, Wessels BW, Siegel JA, Howell RW, et al. MIRD pamphlet No. 17: the dosimetry of nonuniform activity distributions – radionuclide S values at the voxel level. Medical Internal Radiation Dose Committee. J Nucl Med 1999;40:11S–36S.
Pacilio M, Lanconelli N, Lo Meo S, Betti M, Montani L, Torres Aroche LA, et al. Differences among Monte Carlo codes in the calculations of voxel S-values for radionuclide targeted therapy and analysis of their impact on absorbed dose evaluations. Med Phys 2009;36:1543–52.
Hobbs RF, Sgouros G. Calculation of the biological effective dose for piecewise defined dose-rate fits. Med Phys 2009;36:904–7.
Alati T, Van Cleeff M, Strom SC, Jirtle RL. Radiation sensitivity of adult human parenchymal hepatocytes. Radiat Res 1988;1:152–60.
Schultz-Hector S, Sund M, Thames HD. Fractionation response and repair kinetics of radiation-induced heart failure in the rat. Radiother Oncol 1992;1:33–40.
van Rongen E, Travis EL, Thames HD Jr. Repair rate in mouse lung after clinically relevant radiation doses per fraction. Radiat Res 1995;1:74–8.
van Rongen E, Thames HD Jr, Travis EL. Recovery from radiation damage in mouse lung: interpretation in terms of two rates of repair. Radiat Res 1993;2:225–33.
Thames HD, Ang KK, Stewart FA, van Der Schuren E. Does incomplete repair explain the apparent failure of the basic LQ model to predict spinal cord and kidney responses to low doses per fraction? Int J Radiat Biol 1988;54:13–9.
Halperin EC, Perez Carlos AP, Brady LW. Principles and practice of radiation oncology, 5th edn. Philadelphia: Lippincott Williams & Wilkins, Philadelphia; 2008.
Dale RG. Dose-rate effects in targeted radiotherapy. Phys Med Biol 1996;41:1871–84.
Wiseman GA, Leigh BR, Dunn WL, Stabin MG, White CA. Additional radiation absorbed dose estimates for Zevalin™ radioimmunotherapy. Biother Radiopharm 2003;18:253–8.
Assié K, Dieudonné A, Gardin I, Buvat I, Tilly H, Vera P. Comparison between 2D and 3D dosimetry protocols in 90Y-ibritumomab tiuxetan radioimmunotherapy of patients with non-Hodgkin’s lymphoma. Cancer Biother Radiopharm 2008;23:53–65.
He B, Wahl RL, Sgouros G, Du Y, Jacene H, Kasecamp WR, et al. Comparison of organ residence time estimation methods for radioimmunotherapy dosimetry and treatment planning – patient studies. Med Phys 2009;36:1595–601.
He B, Du Y, Segars WP, Wahl RL, Sgouros G, Jacene H, et al. Evaluation of quantitative imaging methods for organ activity and residence time estimation using a population of phantoms having realistic variations in anatomy and uptake. Med Phys 2009;36:612–9.
Hernandez MC, Knox SJ. Radiobiology of radioimmunotherapy: targeting CD20 B-cell antigen in non-Hodgkin’s lymphoma. Int J Radiation Oncol Biol Phys 2004;59:1274–87.
Haas RL, Poortmans P, de Jong D, Aleman BM, Dewit LG, Verheij M, et al. High response rates and lasting remissions after low-dose involved field radiotherapy in indolent lymphomas. J Clin Oncol 2003;21:2474–80.
Haas RL. Low dose radiotherapy in indolent lymphomas, enough is enough. Hematol Oncol 2009;27:71–81.
Author information
Authors and Affiliations
Corresponding author
Appendix: Calculation of the Lea-Catcheside factor for different biokinetics in radionuclide targeted therapy
Appendix: Calculation of the Lea-Catcheside factor for different biokinetics in radionuclide targeted therapy
In many cases, the absorbed dose-rate to the tumour, or to the critical organs, increases from an initial value of zero to some maximum value (uptake phase), and then decreases (clearance phase). According to Howell et al. [10], the presence of an uptake phase can be described by the following functional form for the absorbed dose rate:
where λeff is the effective clearance rate constant and λin is the effective uptake rate constant. By defining the effective clearance half-time (Te) and the effective uptake half-time (Teu), λeff = ln2/Te and λin = ln2/Teu. Following the procedure of Dale [11], Howell et al. [10] calculated the RE when the equation above is used for describing the biokinetics:
In the original equations, the initial dose rate r0 was used, but it was subsequently substituted by the product between the absorbed dose and λeff. In this work, Eq. A2 was used for BED calculations when the biokinetics showed an uptake phase.
Baechler et al. [14] provided a general model for the calculation of the G factor, whatever the number of exponential clearance components or source organs:
where s is the number of source organs, n is the number of clearance exponential components, Sh (or Sm) is the S value from the source organ h (or m), fh (or fm) is the “initial activity fraction” for the source organ h (or m) obtained by extrapolating to zero time a multiexponential expression fitted to the time–activity curve, and ak,m (or ai,h) is the activity fraction coefficient of the k-th (or i-th) exponential clearance component in the multiexponential expression fitted to the time–activity curve. For a unique source with monoexponential clearance (i.e. s = n = 1), G1,1 = λ/(λ+μ), and the resulting RE is identical to that of the Dale formula [38].
For a unique biexponential decaying source, the G factor is derived as follows:
Equation A4 was used here for BED calculations when the biokinetics indicated only clearance phases (e.g. for the lungs). When activity is located in two source organs, considering monoexponential clearance for each one (i.e. s = 2 and n = 1) the factor G2,1 is expressed as follows:
The above equation was used in this work when the contributions from two source organ were taken into account in calculating the BED, i.e. for the red marrow (red marrow and remainder of the body) and the heart wall (heart wall and heart content).
Rights and permissions
About this article
Cite this article
Pacilio, M., Betti, M., Cicone, F. et al. A theoretical dose-escalation study based on biological effective dose in radioimmunotherapy with 90Y-ibritumomab tiuxetan (Zevalin). Eur J Nucl Med Mol Imaging 37, 862–873 (2010). https://doi.org/10.1007/s00259-009-1333-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-009-1333-4