
Abstract
Objective
To evaluate the value of a dedicated interpretation of the CT images in the differential diagnosis of benign vs. malignant primary bone lesions with 18fluorodeoxyglucose-positron emission tomography/computed tomography (18F-FDG-PET/CT).
Materials and methods
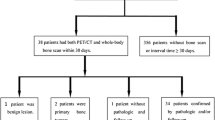
In 50 consecutive patients (21 women, 29 men, mean age 36.9, age range 11–72) with suspected primary bone neoplasm conventional radiographs and 18F-FDG-PET/CT were performed. Differentiation of benign and malignant lesions was separately performed on conventional radiographs, PET alone (PET), and PET/CT with specific evaluation of the CT part. Histology served as the standard of reference in 46 cases, clinical, and imaging follow-up in four cases.
Results
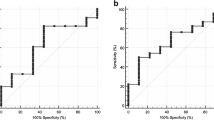
According to the standard of reference, conventional 17 lesions were benign and 33 malignant. Sensitivity, specificity, and accuracy in assessment of malignancy was 85%, 65% and 78% for conventional radiographs, 85%, 35% and 68% for PET alone and 91%, 77% and 86% for combined PET/CT. Median SUVmax was 3.5 for benign lesions (range 1.6–8.0) and 5.7 (range 0.8–41.7) for malignant lesions.
In eight patients with bone lesions with high FDG-uptake (SUVmax ≥ 2.5) dedicated CT interpretation led to the correct diagnosis of a benign lesion (three fibrous dysplasias, two osteomyelitis, one aneurysmatic bone cyst, one fibrous cortical defect, 1 phosphaturic mesenchymal tumor). In four patients with lesions with low FDG-uptake (SUVmax < 2.5) dedicated CT interpretation led to the correct diagnosis of a malignant lesion (three chondrosarcomas and one leiomyosarcoma). Combined PET/CT was significantly more accurate in the differentiation of benign and malignant lesions than PET alone (p = .039). There was no significant difference between PET/CT and conventional radiographs (p = .625).
Conclusion
Dedicated interpretation of the CT part significantly improved the performance of FDG-PET/CT in differentiation of benign and malignant primary bone lesions compared to PET alone. PET/CT more commonly differentiated benign from malignant primary bone lesions compared with conventional radiographs, but this difference was not significant.







Similar content being viewed by others

References
Aquino SL, Kuester LB, Muse VV, Halpern EF, Fischman AJ. Accuracy of transmission CT and FDG-PET in the detection of small pulmonary nodules with integrated PET/CT. Eur J Nucl Med Mol Imaging 2006;33:692–96.
Yi CA, Lee KS, Kim BT, et al. Tissue characterization of solitary pulmonary nodule: comparative study between helical dynamic CT and integrated PET/CT. J Nucl Med 2006;47:443–50.
Sperti C, Pasquali C, Chierichetti F, Liessi G, Ferlin G, Pedrazzoli S. Value of 18-fluorodeoxyglucose positron emission tomography in the management of patients with cystic tumors of the pancreas. Ann Surg 2001;234:675–80.
Pauls S, Buck AK, Halter G, et al. Performance of integrated FDG-PET/CT for differentiating benign and malignant lung lesions—results from a large prospective clinical trial. Mol Imaging Biol 2008;10:121–28.
von Schulthess GK, Steinert HC, Hany TF. Integrated PET/CT: current applications and future directions. Radiology 2006;238:405–22.
Brenner W, Bohuslavizki KH, Eary JF. PET imaging of osteosarcoma. J Nucl Med 2003;44:930–42.
Aoki J, Endo K, Watanabe H, et al. FDG-PET for evaluating musculoskeletal tumors: a review. J Orthop Sci 2003;8:435–41.
Hain SF, O’Doherty MJ, Bingham J, Chinyama C, Smith MA. Can FDG PET be used to successfully direct preoperative biopsy of soft tissue tumours? Nucl Med Commun 2003;24:1139–43.
Schulte M, Brecht-Krauss D, Heymer B, et al. Grading of tumors and tumorlike lesions of bone: evaluation by FDG PET. J Nucl Med 2000;41:1695–701.
Folpe AL, Lyles RH, Sprouse JT, Conrad EU 3rd, Eary JF. (F-18) fluorodeoxyglucose positron emission tomography as a predictor of pathologic grade and other prognostic variables in bone and soft tissue sarcoma. Clin Cancer Res 2000;6:1279–87.
Tateishi U, Yamaguchi U, Seki K, Terauchi T, Arai Y, Kim EE. Bone and soft-tissue sarcoma: preoperative staging with fluorine 18 fluorodeoxyglucose PET/CT and conventional imaging. Radiology 2007;245:839–47.
Hawkins DS, Rajendran JG, Conrad EU 3rd, Bruckner JD, Eary JF. Evaluation of chemotherapy response in pediatric bone sarcomas by [F-18]-fluorodeoxy-d-glucose positron emission tomography. Cancer 2002;94:3277–84.
Schulte M, Brecht-Krauss D, Werner M, et al. Evaluation of neoadjuvant therapy response of osteogenic sarcoma using FDG PET. J Nucl Med 1999;40:1637–43.
Aoki J, Watanabe H, Shinozaki T, et al. FDG PET of primary benign and malignant bone tumors: conventionalized uptake value in 52 lesions. Radiology 2001;219:774–7.
Strobel K, Dummer R, Husarik DB, Perez Lago M, Hany TF, Steinert HC. High-risk melanoma: accuracy of FDG PET/CT with added CT morphologic information for detection of metastases. Radiology 2007;244:566–74.
Delbeke D, Coleman RE, Guiberteau MJ, et al. Procedure guideline for tumor imaging with 18F-FDG PET/CT 1.0. J Nucl Med 2006;47:885–95.
Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F. Determining growth rates of focal lesions of bone from radiographs. Radiology 1980;134:577–83.
Freyschmidt J. [Conventionals and diagnostic strategies in diagnosis of bone tumors and tumor-simulating lesions]. Radiologe 1998;38:287–300.
Resnick D. Tumors and tumor-like lesions of bone: radiographic principles. In: Resnick D, Niwayama G (eds). Diagnosis of bone and joint disorders, 1988 ed. Philadelphia: W.B. Saunders Company; 1988. p. 3603–15.
Bloem JL, Taminiau AH, Eulderink F, Hermans J, Pauwels EK. Radiologic staging of primary bone sarcoma: MR imaging, scintigraphy, angiography, and CT correlated with pathologic examination. Radiology 1988;169:805–10.
Lukens JA, McLeod RA, Sim FH. Computed tomographic evaluation of primary osseous malignant neoplasms. AJR Am J Roentgenol 1982;139:45–8.
Andre M, Resnick D. Computed tomography. In: Resnick D, Niwayama G (eds). Diagnosis of bone and joint disorders. Philadelphia: W.B.Saunders Company; 1988. p. 143–203.
Goodin GS, Shulkin BL, Kaufman RA, McCarville MB. PET/CT characterization of fibroosseous defects in children: 18F-FDG uptake can mimic metastatic disease. AJR Am J Roentgenol 2006;187:1124–8.
Strobel K, Bode B, Lardinois D, Exner U. PET-positive fibrous dysplasia—a potentially misleading incidental finding in a patient with intimal sarcoma of the pulmonary artery. Skeletal Radiol 2007;36(Suppl 1):S24–8.
Daffner RH, Kirks DR, Gehweiler JA Jr, Heaston DK. Computed tomography of fibrous dysplasia. AJR Am J Roentgenol 1982;139:943–8.
Brenner W, Conrad EU, Eary JF. FDG PET imaging for grading and prediction of outcome in chondrosarcoma patients. Eur J Nucl Med Mol Imaging 2004;31:189–95.
Strobel K, Stumpe KD. PET/CT in Musculoskeletal Infection. Semin Musculoskelet Radiol 2007;11:353–64.
Wyss MT, Honer M, Spath N, et al. Influence of ceftriaxone treatment on FDG uptake–an in vivo [18F]-fluorodeoxyglucose imaging study in soft tissue infections in rats. Nucl Med Biol 2004;31:875–82.
Shin DS, Shon OJ, Byun SJ, Choi JH, Chun KA, Cho IH. Differentiation between malignant and benign pathologic fractures with F-18-fluoro-2-deoxy-d-glucose positron emission tomography/computed tomography. Skeletal Radiol 2008;37:415–21.
Schmitz A, Risse JH, Textor J, et al. FDG-PET findings of vertebral compression fractures in osteoporosis: preliminary results. Osteoporos Int 2002;13:755–61.
Kern KA, Brunetti A, Norton JA, et al. Metabolic imaging of human extremity musculoskeletal tumors by PET. J Nucl Med 1988;29:181–6.
Adler LP, Blair HF, Makley JT, et al. Noninvasive grading of musculoskeletal tumors using PET. J Nucl Med 1991;32:1508–12.
Keyes JW Jr. SUV: conventional uptake or silly useless value? J Nucl Med 1995;36:1836–9.
Dehdashti F, Siegel BA, Griffeth LK, et al. Benign versus malignant intraosseous lesions: discrimination by means of PET with 2-[F-18]fluoro-2-deoxy-d-glucose. Radiology 1996;200:243–7.
Adler LP, Blair HF, Makley JT, Pathria MN, Miraldi F. Comparison of PET with CT, MRI, and conventional scintigraphy in a benign and in a malignant soft tissue tumor. Orthopedics 1991;14:891–4. discussion 894–895.
Franzius C, Sciuk J, Daldrup-Link HE, Jurgens H, Schober O. FDG-PET for detection of osseous metastases from malignant primary bone tumours: comparison with bone scintigraphy. Eur J Nucl Med 2000;27:1305–11.
Horger M, Bares R. The role of single-photon emission computed tomography/computed tomography in benign and malignant bone disease. Semin Nucl Med 2006;36:286–94.
Bruzzi JF, Macapinlac H, Tsimberidou AM, et al. Detection of Richter’s transformation of chronic lymphocytic leukemia by PET/CT. J Nucl Med 2006;47:1267–73.
Yalniz E, Er T, Ozyilmaz F. Fibrous dysplasia of the spine with sarcomatous transformation: a case report and review of the literature. Eur Spine J 1995;4:372–4.
Eary JF, Conrad EU. PET imaging: update on sarcomas. Oncology (Williston Park) 2007;21:249–52.
Gerth HU, Juergens KU, Dirksen U, Gerss J, Schober O, Franzius C. Significant benefit of multimodal imaging: PET/CT compared with PET alone in staging and follow-up of patients with Ewing tumors. J Nucl Med 2007;48:1932–9.
Lodge MA, Lucas JD, Marsden PK, Cronin BF, O’Doherty MJ, Smith MA. A PET study of 18FDG uptake in soft tissue masses. Eur J Nucl Med 1999;26:22–30.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Strobel, K., Exner, U.E., Stumpe, K.D.M. et al. The additional value of CT images interpretation in the differential diagnosis of benign vs. malignant primary bone lesions with 18F-FDG-PET/CT. Eur J Nucl Med Mol Imaging 35, 2000–2008 (2008). https://doi.org/10.1007/s00259-008-0876-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-008-0876-0