
Abstract
Objective
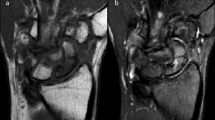
To assess dynamic contrast-enhanced magnetic resonance imaging (DCE MRI) as a measure of vascularity in scaphoid delayed-union or non-union.
Materials and methods
Thirty-five patients (34 male, one female; mean age, 27.4 ± 9.4 years; range, 16–51 years) with scaphoid delayed-union and non-union who underwent DCE MRI of the scaphoid between September 2002 and October 2012 were retrospectively reviewed. Proximal fragment vascularity was classified as good, fair, or poor on unenhanced MRI, contrast-enhanced MRI, and DCE MRI. For DCE MRI, enhancement slope, Eslope comparison of proximal and distal fragments was used to classify the proximal fragment as good, fair, or poor vascularity. Proximal fragment vascularity was similarly graded at surgery in all patients. Paired t test and McNemar test were used for data comparison. Kappa value was used to assess level of agreement between MRI findings and surgical findings.
Results
Twenty-five (71 %) of 35 patients had good vascularity, four (11 %) had fair vascularity, and six (17 %) had poor vascularity of the proximal scaphoid fragment at surgery. DCE MRI parameters had the highest correlation with surgical findings (kappa = 0.57). Proximal scaphoid fragments with surgical poor vascularity had a significantly lower Emax and Eslope than those with good vascularity (p = 0.0043 and 0.027). The sensitivity, specificity, positive and negative predictive value and accuracy of DCE MRI in predicting impaired vascularity was 67, 86, 67, 86, and 80 %, respectively, which was better than that seen with unenhanced and post-contrast MRI. Flattened time intensity curves in both proximal and distal fragments were a feature of protracted non-union with a mean time interval of 101.6 ± 95.5 months between injury and MRI.
Conclusions
DCE MRI has a higher diagnostic accuracy than either non-enhanced MRI or contrast enhanced MRI for assessing proximal fragment vascularity in scaphoid delayed-union and non-union. For proper interpretation of contrast-enhanced studies in scaphoid vascularity, one needs to incorporate the time frame between injury and MRI.





Similar content being viewed by others


References
Hove LM. Epidemiology of scaphoid fractures in Bergen, Norway. Scand J Plast Reconstr Surg Hand Surg. 1999;33:423–6.
Larsen CF, Brøndum V, Skov O. Epidemiology of scaphoid fractures in Odense, Denmark. Acta Orthop Scand. 1992;63:216–8.
Gelberman RH, Wolock BS, Siegel DB. Fractures and non-unions of the carpal scaphoid. J Bone Joint Surg Am. 1989;71:1560–5.
Taleisnik J, Kelly PJ. The extraosseous and intraosseous blood supply of the scaphoid bone. J Bone Joint Surg Am. 1966;48:1125–37.
Dawson JS, Martel AL, Davis TR. Scaphoid blood flow and acute fracture healing. A dynamic MRI study with enhancement with gadolinium. J Bone Joint Surg Br. 2001;83:809–14.
Steinmann SP, Adams JE. Scaphoid fractures and nonunions: diagnosis and treatment. J Orthop Sci. 2006;11:424–31.
Anderson SE, Steinbach LS, Tschering-Vogel D, Martin M, Nagy L. MR imaging of avascular scaphoid nonunion before and after vascularized bone grafting. Skeletal Radiol. 2005;34:314–20.
Perlik PC, Guilford WB. Magnetic resonance imaging to assess vascularity of scaphoid nonunions. J Hand Surg Am. 1991;16:479–84.
Green DP. The effect of avascular necrosis on Russe bone grafting for scaphoid nonunion. J Hand Surg Am. 1985;10:597–605.
Inoue G, Shionoya K, Kuwahata Y. Ununited proximal pole scaphoid fractures. Treatment with a Herbert screw in 16 cases followed for 0.5–8 years. Acta Orthop Scand. 1997;68:124–7.
Robbins RR, Ridge O, Carter PR. Iliac crest bone grafting and Herbert screw fixation of nonunions of the scaphoid with avascular proximal poles. J Hand Surg Am. 1995;20:818–31.
Fernandez DL, Eggli S. Non-union of the scaphoid. Revascularization of the proximal pole with implantation of a vascular bundle and bone-grafting. J Bone Joint Surg Am. 1995;77:883–93.
Fox MG, Gaskin CM, Chhabra AB, Anderson MW. Assessment of scaphoid viability with MRI: a reassessment of findings on unenhanced MR images. AJR Am J Roentgenol. 2010;195:W281–6.
Sakuma M, Nakamura R, Imaeda T. Analysis of proximal fragment sclerosis and surgical outcome of scaphoid non-union by magnetic resonance imaging. J Hand Surg Br. 1995;20:201–5.
Büchler U, Nagy L. The issue of vascularity in fractures and non-union of the scaphoid. J Hand Surg Br. 1995;20:726–35.
Cerezal L, Abascal F, Canga A, García-Valtuille R, Bustamante M, del Piñal F. Usefulness of gadolinium-enhanced MR imaging in the evaluation of the vascularity of scaphoid nonunions. AJR Am J Roentgenol. 2000;174:141–9.
Schmitt R, Christopoulos G, Wagner M, Krimmer H, Fodor S, van Schoonhoven J, et al. Avascular necrosis (AVN) of the proximal fragment in scaphoid nonunion: is intravenous contrast agent necessary in MRI? Eur J Radiol. 2011;77:222–7.
Megerle K, Worg H, Christopoulos G, Schmitt R, Krimmer H. Gadolinium-enhanced preoperative MRI scans as a prognostic parameter in scaphoid nonunion. J Hand Surg Eur. 2011;36:23–8.
Singh AK, Davis TR, Dawson JS, Oni JA, Downing ND. Gadolinium enhanced MR assessment of proximal fragment vascularity in nonunions after scaphoid fracture: does it predict the outcome of reconstructive surgery? J Hand Surg Br. 2004;29:444–8.
Donati OF, Zanetti M, Nagy L, Bode B, Schweizer A, Pfirrmann CW. Is dynamic gadolinium enhancement needed in MR imaging for the preoperative assessment of scaphoidal viability in patients with scaphoid nonunion? Radiology. 2011;260:808–16.
Kim JK, Kim JO, Lee SY. Volar percutaneous screw fixation for scaphoid waist delayed union. Clin Orthop Relat Res. 2010;468(4):1066–71.
Wong WY, Ho PC. Minimal invasive management of scaphoid fractures: from fresh to nonunion. Hand Clin. 2011;27:291–307.
Cova M, Kang YS, Tsukamoto H, et al. Bone marrow perfusion evaluated with gadolinium-enhanced dynamic fast MR imaging in a dog model. Radiology. 1991;179:535–9.
Konishiike T, Makihata E, Tago H, Sato T, Inoue H. Acute fracture of the neck of the femur. An assessment of perfusion of the head by dynamic MRI. J Bone Joint Surg Br. 1999;81:596–9.
Waitayawinyu T, Pfaeffle HJ, McCallister WV, Nemechek NM, Trumble TE. Management of scaphoid nonunions. Hand Clin. 2010;26:105–17.
Ciprian S, Iochum S, Kohlmann R, Dautel G, Dap F, Blum A. MR imaging accuracy in the prediction of bone graft healing potential in scaphoid non-union. J Radiol. 2004;85:1699–706.
Sunagawa T, Bishop AT, Muramatsu K. Role of conventional and vascularized bone grafts in scaphoid nonunion with avascular necrosis: a canine experimental study. J Hand Surg Am. 2000;25:849–59.
Sakai T, Sugano N, Nishii T, Haraguchi K, Ochi T, Ohzono K. MR findings of necrotic lesions and the extralesional area of osteonecrosis of the femoral head. Skeletal Radiol. 2000;29:133–41.
Griffith JF, Antonio GE, Kumta SM, Hui DS, Wong JK, Joynt GM, et al. Osteonecrosis of hip and knee in patients with severe acute respiratory syndrome treated with steroids. Radiology. 2005;235:168–75.
Vande Berg B, Malghem J, Labaisse MA, Noel H, Maldague B. Avascular necrosis of the hip: comparison of contrast-enhanced and nonenhanced MR imaging with histologic correlation. Work in progress. Radiology. 1992;182:445–50.
Reinus WR, Conway WF, Totty WG, Gilula LA, Murphy WA, Siegel BA, et al. Carpal avascular necrosis: MR imaging. Radiology. 1986;160:689–93.
Urban MA, Green DP, Aufdemorte TB. The patchy configuration of scaphoid avascular necrosis. J Hand Surg Am. 1993;18:669–74.
Desser TS, McCarthy S, Trumble T. Scaphoid fractures and Kienbock’s disease of the lunate: MR imaging with histopathologic correlation. Magn Reson Imaging. 1990;8:357–61.
Dailiana ZH, Zachos V, Varitimidis S, Papanagiotou P, Karantanas A, Malizos KN. Scaphoid nonunions treated with vascularised bone grafts: MRI assessment. Eur J Radiol. 2004;50:217–24.
Erlemann R, Reiser MF, Peters PE, Vasallo P, Nommensen B, Kusnierz-Glaz CR, et al. Musculoskeletal neoplasms: static and dynamic Gd-DTPA–enhanced MR imaging. Radiology. 1989;171:767–73.
Griffith JF, Kumta SM, Huang Y. Hard arteries, weak bones. Skeletal Radiol. 2011;40:517–21.
Müller M, Germann G, Sauerbier M. Minimal invasive screw fixation and early mobilization of acute scaphoid fractures in the middle third: operative technique and early functional outcome. Tech Hand Up Extrem Surg. 2008;12:107–13.
Acknowledgments
The work described in this paper was partially supported by a grant from the Research Grants Council of the Hong Kong Special Administrative Region, China (Project No.SEG_CUHK02). Special thanks to Jason Leung, CUHK statistician, for his help with this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ng, A.W.H., Griffith, J.F., Taljanovic, M.S. et al. Is dynamic contrast-enhanced MRI useful for assessing proximal fragment vascularity in scaphoid fracture delayed and non-union?. Skeletal Radiol 42, 983–992 (2013). https://doi.org/10.1007/s00256-013-1627-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-013-1627-2