
Abstract
Objective
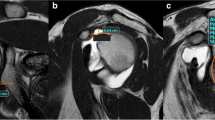
The purpose of this study was primarily to assess the diagnostic performance of magnetic resonance imaging (MRI) in detecting articular cartilage injuries in patients with glenohumeral instability. A secondary purpose was to assess the diagnostic performance of MRI for detection of Hill–Sachs and Bankart lesions.
Materials and Methods
A cohort of 87 consecutive patients who underwent diagnostic MRI and shoulder arthroscopy for instability from 1997 to 2006 were identified. Fifty-five patients (63.2%) underwent MRI with intra-articular contrast medium and 32 patients (36.8%) underwent MRI without contrast medium. MR images were reviewed by two radiologists and interpreted by consensus for the presence of articular cartilage lesions (including Hill–Sachs and Bankart lesions), which were then confirmed by reviewing the operative report and images recorded at arthroscopy.
Results
Mean patient age was 27.0 ± 10.2 years with a mean clinical and radiographic follow-up of 29 (range 3–72) months. Cartilage injuries were detected arthroscopically in 55 patients (63%). Bankart and Hill–Sachs lesions were identified arthroscopically in 66 patients (75.9%) and 55 patients (63.2%) respectively. The overall sensitivity and specificity for detection of glenohumeral articular cartilage lesions by MRI were 87.2% and 80.6% respectively. The sensitivity and specificity of MRI in detecting Bankart lesions was 98.4% (95% CI 91.9, 99.7) and 95.2% (95% CI 77.3, 99.2) respectively. The sensitivity and specificity of MRI in detecting Hill–Sachs lesions was 96.3% (95% CI 87.6, 98.9%) and 90.6% (95% CI 75.7, 96.9) respectively. No statistically significant difference was found between MRI examinations with and without intra-articular gadolinium (p = 0.89).
Conclusion
Magnetic resonance imaging demonstrates high sensitivity and specificity for the diagnosis of articular cartilage injuries in patients with glenohumeral instability. MRI with or without intra-articular contrast medium in this study were equally reliable as a non-invasive method for assessment of articular cartilage damage of the glenohumeral joint prior to diagnostic arthroscopy.

Similar content being viewed by others


References
Messner K, Gillquist J. Cartilage repair. A critical review [see comment]. Acta Orthop Scand. 1996;67:523–9.
Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L. Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation [see comment]. N Engl J Med. 1994;331:889–95.
O’Driscoll SW. The healing and regeneration of articular cartilage. J Bone Jt Surg Am. 1998;80:1795–812.
Mori R, Ochi M, Sakai Y, Adachi N, Uchio Y. Clinical significance of magnetic resonance imaging (MRI) for focal chondral lesions. Magn Reson Imaging. 1999;17:1135–40.
Recht MP, Piraino DW, Paletta GA, Schils JP, Belhobek GH. Accuracy of fat-suppressed three-dimensional spoiled gradient-echo FLASH MR imaging in the detection of patellofemoral articular cartilage abnormalities. Radiology. 1996;198:209–12.
Samilson RL, Prieto V. Dislocation arthropathy of the shoulder. J Bone Jt Surg Am. 1983;65:456–60.
Outerbridge RE, Dunlop JA. The problem of chondromalacia patellae. Clin Orthop Relat Res 1975;(110:)177–96.
Outerbridge RE. The etiology of chondromalacia patellae. 1961. Clin Orthop Relat Res. 2001;(389):5–8.
Cameron ML, Briggs KK, Steadman JR. Reproducibility and reliability of the Outerbridge classification for grading chondral lesions of the knee arthroscopically. Am J Sports Med. 2003;31:83–6.
Anderson WJ, Guilford WB. Osteochondritis dissecans of the humeral head. An unusual cause of shoulder pain. Clin Orthop Relat Res. 1983;(173):166–8.
Johnson DL, Warner JJ. Osteochondritis dissecans of the humeral head: treatment with a matched osteochondral allograft. J Shoulder Elbow Surg. 1997;6:160–3.
Yeh LR, Kwak S, Kim YS, et al. Evaluation of articular cartilage thickness of the humeral head and the glenoid fossa by MR arthrography: anatomic correlation in cadavers. Skeletal Radiol. 1998;27:500–4.
Denti M, Monteleone M, Trevisan C, De Romedis B, Barmettler F. Magnetic resonance imaging versus arthroscopy for the investigation of the osteochondral humeral defect in anterior shoulder instability. A double-blind prospective study. Knee Surg Sports Traumatol Arthrosc. 1995;3:184–6.
Kreitner KF, Loew R, Runkel M, Zollner J, Thelen M. Low-field MR arthrography of the shoulder joint: technique, indications, and clinical results. Eur Radiol. 2003;13:320–9.
Volpi D, Olivetti L, Budassi P, Genovese E. Capsulo-labro-ligamentous lesions of the shoulder: evaluation with MR arthrography. Radiol Med. 2003;105:162–70.
Gusmer PB, Potter HG. Imaging of shoulder instability. Clin Sports Med. 1995;14:777–95.
Guntern DV, Pfirrmann CW, Schmid MR, et al. Articular cartilage lesions of the glenohumeral joint: diagnostic effectiveness of MR arthrography and prevalence in patients with subacromial impingement syndrome. Radiology. 2003;226:165–70.
Probyn LJ, White LM, Salonen DC, Tomlinson G, Boynton EL. Recurrent symptoms after shoulder instability repair: direct MR arthrographic assessment—correlation with second-look surgical evaluation. Radiology. 2007;245:814–23.
Disclaimer
Diane L. Dahm, Meredith L. Hayes, Mark S. Collins, Doris E. Wegner, and Joseph A. Morgan: These authors, their immediate family, and any research foundation with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article.
Author information
Authors and Affiliations
Corresponding author
Additional information
Investigation performed at the Mayo Clinic, Rochester, MN, USA. Mayo Clinic IRB No. 06-002671
Rights and permissions
About this article
Cite this article
Hayes, M.L., Collins, M.S., Morgan, J.A. et al. Efficacy of diagnostic magnetic resonance imaging for articular cartilage lesions of the glenohumeral joint in patients with instability. Skeletal Radiol 39, 1199–1204 (2010). https://doi.org/10.1007/s00256-010-0922-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-010-0922-4