
Abstract
Background
Stages of healing for classic metaphyseal lesions (CMLs) are not well established. Follow-up skeletal surveys provide an opportunity to evaluate signs of healing CMLs.
Objective
To evaluate the sequence of CML healing phases by comparing initial and follow-up skeletal surveys in children with distal tibial CMLs on the initial survey. Findings could assist in child abuse investigations.
Materials and methods
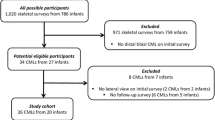
We identified all distal tibia CMLs with initial and follow-up skeletal surveys performed January 2009 through December 2018 at our institution. Two pediatric radiologists reviewed the surveys using Likert score from 1 (no CML) to 5 (definite CML). Only cases with score of 4 or 5 by both radiologists were selected for the study. The initial and 2-week follow-up skeletal surveys were reviewed in consensus for presence of the following signs: corner fracture, thin bucket handle fracture, thick bucket handle fracture, bucket handle fracture with endochondral bone filling the gap, subphyseal lucency, deformed corner, and subperiosteal new bone formation. We used the Kruskal–Wallis test to evaluate for significant difference in thickness among thin bucket handle fracture, thick bucket handle fracture, and bucket handle fracture with endochondral bone filling the gap.
Results
We included 26 children (12 girls) with age range 1–9.9 months who had a combined 34 distal tibia CMLs. Thin bucket handle fracture (n=13, 38.2%) was only seen on initial survey. On follow-up, six children had thick bucket handle fracture and four had bucket handle fracture with endochondral bone filling the gap. Fourteen thick bucket handle fractures (n=9) or bucket handle fractures with endochondral bone filling the gap (n=5) were noted on initial surveys; on follow-up, three (21.4%) had deformed corner, one (7.1%) had corner fracture, one (7.1%) had subphyseal lucency, and five (35.7%) were normal. None demonstrated thin bucket handle fracture on follow-up. Two of the nine (22.2%) thick bucket handle fractures became thicker, and 3/9 (33.3%) became bucket handle fractures with endochondral bone filling the gap. The metaphysis normalized in 8/34 (23.5%) CMLs on follow-up surveys. The thickness of thin bucket handle fracture was less than 1 mm (mean±standard deviation [SD] = 0.6±0.2 mm), which was significantly thinner (P<0.0001) compared with thick bucket handle fracture (1.7±0.5 mm) and bucket handle fracture with endochondral bone filling the gap (1.9±0.6 mm).
Conclusion
The lack of thin bucket handle fractures on any follow-up skeletal surveys suggests this sign represents an acute phase of injury. The next phases of healing appear to be thick bucket handle fracture followed by bucket handle fracture with endochondral bone filling the gap. It is important to note that normalization of the metaphysis at 2-week follow-up does not exclude CML because this was seen in about one-fifth of cases.








Similar content being viewed by others


References
Wood JN, Fakeye O, Feudtner C et al (2014) Development of guidelines for skeletal survey in young children with fractures. Pediatrics 134:45–53
Wood JN, Fakeye O, Mondestin V et al (2015) Development of hospital-based guidelines for skeletal survey in young children with bruises. Pediatrics 135:e312–e320
Prosser I, Lawson Z, Evans A et al (2012) A timetable for the radiologic features of fracture healing in young children. AJR Am J Roentgenol 198:1014–1020
Islam O, Soboleski D, Symons S et al (2000) Development and duration of radiographic signs of bone healing in children. AJR Am J Roentgenol 175:75–78
Fadell M, Miller A, Trefan L et al (2017) Radiological features of healing in newborn clavicular fractures. Eur Radiol 27:2180–2187
Halliday KE, Broderick NJ, Somers JM et al (2011) Dating fractures in infants. Clin Radiol 66:1049–1054
Berkowitz CD (2017) Physical abuse of children. N Engl J Med 376:1659–1666
Flaherty EG, Perez-Rossello JM, Levine MA et al (2014) Evaluating children with fractures for child physical abuse. Pediatrics 133:e477–e489
Kleinman PK, Perez-Rossello JM, Newton AW et al (2011) Prevalence of the classic metaphyseal lesion in infants at low versus high risk for abuse. AJR Am J Roentgenol 197:1005–1008
Tsai A, Connolly SA, Ecklund K et al (2019) Subperiosteal new bone formation with the distal tibial classic metaphyseal lesion: prevalence on radiographic skeletal surveys. Pediatr Radiol 49:551–558
Kleinman PK, Marks SC Jr, Spevak MR et al (1991) Extension of growth-plate cartilage into the metaphysis: a sign of healing fracture in abused infants. AJR Am J Roentgenol 156:775–779
Offiah A, van Rijn RR, Perez-Rossello JM et al (2009) Skeletal imaging of child abuse (non-accidental injury). Pediatr Radiol 39:461–470
Walters MM, Forbes PW, Buonomo C et al (2014) Healing patterns of clavicular birth injuries as a guide to fracture dating in cases of possible infant abuse. Pediatr Radiol 44:1224–1229
Adamsbaum C, Mejean N, Merzoug V et al (2010) How to explore and report children with suspected non-accidental trauma. Pediatr Radiol 40:932–938
Paddock M, Sprigg A, Offiah AC (2017) Imaging and reporting considerations for suspected physical abuse (non-accidental injury) in infants and young children. Part 1: initial considerations and appendicular skeleton. Clin Radiol 72:179–188
Kleinman PK (2008) Problems in the diagnosis of metaphyseal fractures. Pediatr Radiol 38:S388–S394
Tsai A, McDonald AG, Rosenberg AE et al (2014) High-resolution CT with histopathological correlates of the classic metaphyseal lesion of infant abuse. Pediatr Radiol 44:124–140
Kleinman PK, Marks SC Jr (1996) A regional approach to the classic metaphyseal lesion in abused infants: the proximal tibia. AJR Am J Roentgenol 166:421–426
Kleinman PK, Marks SC Jr (1996) A regional approach to the classic metaphyseal lesion in abused infants: the proximal humerus. AJR Am J Roentgenol 167:1399–1403
Kleinman PK, Marks SC Jr (1996) A regional approach to classic metaphyseal lesions in abused infants: the distal tibia. AJR Am J Roentgenol 166:1207–1212
Kleinman PK, Marks SC Jr (1998) A regional approach to the classic metaphyseal lesion in abused infants: the distal femur. AJR Am J Roentgenol 170:43–47
Osier LK, Marks SC Jr, Kleinman PK (1993) Metaphyseal extensions of hypertrophied chondrocytes in abused infants indicate healing fractures. J Pediatr Orthop 13:249–254
Harper NS, Eddleman S, Lindberg DM (2013) The utility of follow-up skeletal surveys in child abuse. Pediatrics 131:e672–e678
American College of Radiology, Society for Pediatric Radiology (2016) ACR–SPR practice parameter for the performance and interpretation of skeletal surveys in children. https://www.acr.org/-/media/ACR/Files/Practice-Parameters/Skeletal-Survey.pdf. Accessed 9 Dec 2019
Zimmerman S, Makoroff K, Care M et al (2005) Utility of follow-up skeletal surveys in suspected child physical abuse evaluations. Child Abuse Negl 29:1075–1083
Tsai A, Stamoulis C, Barber I, Kleinman PK (2017) Infant lower extremity long bone growth rates: comparison of contemporary with early 20th century data using mixed effect models. Hum Biol 29:e22905
Anderson M, Green WT, Messner MB (1963) Growth and predictions of growth in the lower extremities. J Bone Joint Surg Am 45:1–14
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Karmazyn, B., Marine, M.B., Wanner, M.R. et al. Establishing signs for acute and healing phases of distal tibial classic metaphyseal lesions. Pediatr Radiol 50, 715–725 (2020). https://doi.org/10.1007/s00247-020-04615-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-020-04615-2