
Abstract
Objective
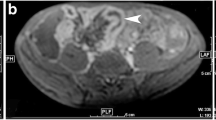
To assess the ability of MRI to detect bowel abnormalities in children affected by Crohn's disease (CD).
Materials and methods
We studied 22 children (age range 8–18 years) referred to us with a known history of CD. MRI was carried out using a 1.5-T unit with a maximum gradient field strength of 16 mT and a phased-array body coil. The sequences performed were breath-hold coronal and axial T2-weighted, express fat saturation, followed by T1-weighted, spoiled gradient, fast fat saturation after IV injection of gadolinium chelate (0.3 mmol/kg) for contrast enhancement of the bowel wall. Bowel distension was achieved using oral administration of isosmotic polyethylene glycol solution. Ileo-colonoscopy was considered the gold standard for evaluation of superficial abnormalities and stenoses of the colon and terminal ileum. MRI findings of bowel-wall thickening, increased vascularisation and extramural involvement were compared with the findings using B-mode and Doppler US. Concordance between MRI and endoscopy, B-mode US and Doppler US findings was determined by the Kappa statistical method.
Results
Superficial lesions were not shown by MRI. MR enteroclysis easily detected stenoses, thickening and hyperaemia of bowel wall. Concordance of findings between MRI and endoscopy was 90% (K=0.79, substantial concordance). Concordance of findings between MRI and US concerning bowel-wall thickening and increased vascularisation was 95% (K=0.875, excellent concordance) and 80% (K=0.6, fairly good concordance), respectively.
Conclusions
Our initial results show that MRI can detect intra- and extra-mural lesions of CD. The high concordance observed between MRI, endoscopy, US and Doppler US findings suggests that MRI is at least comparable for diagnostic capability with these techniques offering, thanks to multiplanar projections, an improved visualisation of the bowel without ionising radiation.







Similar content being viewed by others


References
Goldberg HI, Caruthers SB, Nelson JA, et al (1979) Radiographic findings of the National Cooperative Crohn's disease study. Gastroenterology 77:925–937
Rubesin SE, Scotiniotis I, Birnbaum BA, et al (2001) Radiologic and endoscopic diagnosis of Crohn's disease. Surg Clin North Am 81:39–70
Debatin JF, Patak MA (1999) MRI of the small and large bowel. Eur Radiol 9:1523–1534
Prassopoulos P, Papanikolau N, Grammatikakis J, et al (2001) MR enteroclysis imaging of Crohn disease. Radiographics 21:161–172
Landis JH, Koch GG (1977) The measurement of observer agreement for categorical data (1977) Biometrics 33:159–174
Spalinger J, Patriquin H, Miron MC, et al (2000) Doppler US in patients with Crohn's disease: vessel density in the diseased bowel reflects disease activity. Radiology 217:787–791
Goldberg HI, Gore RM, Margulis AR, et al (1983) Computed tomography in the evaluation of Crohn's disease. AJR 140:277–282
Sarrazin J, Wilson SR (1996) Manifestations of Crohn disease at US. Radiographics 16:499–520
Gore RM, Balthazar EJ, Ghahremani GG, et al (1996) CT features of ulcerative colitis and Crohn's disease. AJR 167:3–15
Mazzeo S, Caramella D, Battolla L, et al (2001) Crohn disease of the small bowel: spiral CT evaluation after oral hyperhydration with isotonic solution. J Comput Assist Tomogr 25:612–616
Potthast S, Rieber A, von Tirpitz C, et al (2002) Ultrasound and magnetic resonance imaging in Crohn's disease: a comparison. Eur Radiol 12:1416–1422
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented at the 39th Congress of the ESPR, Bergen, Norway, June 2002
Rights and permissions
About this article
Cite this article
Magnano, G., Granata, C., Barabino, A. et al. Polyethylene glycol and contrast-enhanced MRI of Crohn's disease in children: preliminary experience. Ped Radiol 33, 385–391 (2003). https://doi.org/10.1007/s00247-003-0903-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-003-0903-z