
Abstract
While swimming represents a popular recreational activity, the immersion of the human body into the water requires a complex physiologic adaption of the whole cardiopulmonary and circulatory system. While this sport is regarded as beneficial, especially in cardiovascular patients, current guidelines hypothesized a possible hazardous effect of swimming and especially diving in patients with univentricular hearts after Fontan palliation. Yet, actual data to underline or contradict these assumptions are lacking. Therefore, this study aimed to conduct a first feasibility study for the evaluation of these effects on Fontan physiology and elucidate the gap of evidence currently preventing patients after Fontan palliation from being restricted from swimming or diving on doctoral advice. Patients recruited from the Heart Center Leipzig, Department of pediatric cardiology, underwent spiroergometry treadmill testing followed by a spiroergometry swimming stress test in a counter current pool. Physiologic data were recorded. A short apnea diving test was performed. The current study found similar physiologic reactions comparing treadmill and swimming exercise stress testing. Heart rate response and oxygen uptake were comparable on land and in the water. This study presents the first-in-man data on swimming and diving in Fontan patients. In this small study cohort of three Fontan patients, there were no adverse events triggered by swimming and breath-hold diving seen. Basically, the physiologic response to exercise was comparable on land and in the water.
Similar content being viewed by others

Introduction
Swimming is a popular recreational activity, representing an effective option in maintaining and improving cardiovascular fitness in healthy people. In this regard, especially cardiovascular patients might profit from this sport. Yet, swimming is also a unique form of exercise, differing from land-based exercises in many aspects [1]. Water immersion places increased pressure on the body, resulting in a rise of pressure in the capacitance vessels with an augmentation of venous return resulting in an increased preload [2, 3]. Left and right heart filling pressures including central venous, right ventricular end-diastolic, left atrial, and left ventricular end-diastolic pressures increase. Left and right ventricular stroke volume increase according to the Starling mechanism by as much as 75–120 cc, with a resulting increase in cardiac output by 30–60%. A various degree of heart rate reduction occurs [4]. Depending on water temperature a variable degree of vasoconstriction at the moment of immersion can be observed, enlarging the left ventricular afterload [5, 6]. Disruptive factors to these complex physiologic mechanisms of adaption to immersion may result in harmful if not life-threatening complications like acute heart failure or swimming-induced pulmonary edema (SIPE). This is also reflected by the current ESC guidelines on sports cardiology, stating that aquatic exercise is not recommended for individuals with heart failure [7].
While there are only incomplete data on physiologic effects of swimming and apnea diving in healthy people, this is particularly of relevance in patients with congenital heart disease after univentricular (Fontan) palliation. To the authors´ knowledge, there are no studies investigating the effects of immersion or submersion on the cardiopulmonary function in Fontan patients. Therefore, this study aimed to conduct a first feasibility study for the evaluation of these effects on Fontan physiology and elucidate the gap of evidence currently preventing generations of congenital heart disease patients after Fontan palliation from being restricted from swimming or diving on doctoral advice.
Methods
Patient selection: Patient recruitment was done by checking the database of the Heart Center Leipzig, Department of Pediatric. Inclusion criteria were age 16 to 25 years, surgical palliation with Fontan, modified Fontan or total cavopulmonary connection (TCPC). Exclusion criteria were severely reduced systemic ventricular ejection fraction, signs of failing Fontan, implanted rhythm devices, severe congestive heart failure neurologic disorders that might prevent free informed consent from the patient. Patients were asked to give informed consent.
Anthropometric data: Body impedance measurement was performed in all patients.
Baseline cardiologic parameters: Patient history, physical examination and a 12-lead ECG, were performed in all patients.
Transthoracic echocardiography: All patients received a complete transthoracic echocardiographic examination (Vivid™ T9, GE Healthcare, Chicago, Illinois, USA). Eyeball assessment and analysis of global peak systolic longitudinal strain were used to describe systolic function of the univentricular hearts. Valvular regurgitation was assessed by semiquantitative color Doppler analysis.
Baseline pulmologic parameters: A spirometry and body plethysmography were performed in all patients.
Treadmill exercise stress test: All patients underwent treadmill exercise stress testing using a modified Balke ramp protocol to reach full exertion [8]. The ramp protocol started with a speed of 2.7 km/h at 0% incline and was increased stepwise every 2 min by 1.4 km/h and 2% incline until full exertion was reached. For patient three, the protocol was adapted to a lower incline of only 1% each step to achieve a proper test duration, as the patient was in reduced physical shape. ECG was recorded continuously. Measurements of respiratory gases were performed using the Cortex METAMAX 3B (R2) spiroergometer. Lactate values were recorded at rest / maximum exertion / 3, 5, 7, and 10 min post exertion.
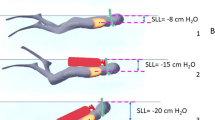
Measurements on diving reflex and oximetry: Patients underwent continuous pulse oximetry 2 min before entering the pool, 2 min while standing in the pool immersed up to the neck, during a short breath-holding dive and 2 min after the dive. Transcutaneous oxygen saturation, heart rate, and perfusion index, as an index of peripheral vascular tone, were recorded.
Swimming exercise stress test: The swimming exercise test was performed following the treadmill stress testing after a rest of 3 h for recovery. The swimming exercise test was performed in a complex setup including a counter current pool, normally used for assessment and training of German Olympic athletes. Extensive precaution safety measures were taken. These included medical staff with two intensive care nurses, two ICU physicians and one rescue diver who remained in the pool during the swimming test, along with full advanced life support equipment on sight. The test was designed and conducted by two sports scientists. Surveillance of counter current speed, water temperature, video surveillance of participants, and spiroergometry during the swim were done. The water temperature was 28° degrees Celsius. The relatively high water temperature was chosen to minimize the patients risk for possible excessive increase in afterload with lower water temperatures. The patients had to complete a ramp protocol. As a protocol we used an institutional approach. The starting speed of the counter current was selected empirically after a short test swim of an untrained healthy female individual from the study team. The duration of 4 min per stage was derived from standard ramp protocol, as commonly used in sports science. 4 min are thought to represent a reasonable time to achieve a cardiovascular steady state at a certain work load. Starting with a counter current of 0.2 m/s for 4 min that was increased to 0.4 m/s for 4 min and lastly 0.5 m/s until full exertion. Measurements of respiratory gases were performed using the swim option for the Cortex METAMAX 3B (R2) spiroergometer. This actual spiroergometer allows the physician to conduct a “normal” spiroergometry during a swim test. Lactate values were recorded at rest / after 4 min of low-intensity swimming / 4 min of moderate-intensity swimming / at maximum exertion / 3 and 5 min post exertion. Blood was taken by a nurse from the left earlobe, while the patients remained immersed in the pool.
One patient agreed to perform a 10 m breath-holding dive followed by a static apnea as long as tolerated. Transcutaneous oxygen saturation, heart rate, and perfusion index were recorded.
Results
Patient Characteristics
Overall 3 patients were included into the study. Patients´ baseline and test characteristics are shown in the following section. Patient selection was hindered by the fact that only few patients felt comfortable enough in the water to perform a swimming exercise stress test. About 30% of contacted Fontan patients stated that they had never learned swimming. In addition, only individuals below 25 years of age could be included due to insurance reasons. Potential additional cardiovascular disease apart from the congenital heart disease was suspected by the insurance company.
Table 1 shows the baseline characteristics.
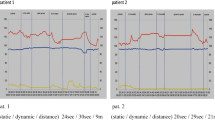
Following, the comparison of treadmill versus the swimming stress testing is shown in Figs. 1, 2, and 3. Patient 1 and 2 showed an apparently similar rise in oxygen uptake (\(\dot{V}O_{2}\)) and carbon dioxide output (\(\dot{V}CO_{2}\)). Heart rate incline seems to be a little steeper in the swimming stress testing. Recognizably, swimming stress testing curves include a short interruption after 4 and 8 min of exercise, reflecting the lactate measurement. Patient 3 suffered from ectopic atrial tachycardia, that was present in the treadmill stress test from minute 8 and in the swimming stress testing from minute 2. Due to a fluctuating 1:1 till 3:1 conduction to the ventricles, the heart rate fluctuates too. While the patient managed to finish the first 4 min of the swimming exercise test, the second 4 min interval had to be interrupted several times as a close evaluation of the physical status of the patient was necessary in the presence of the arrhythmia.

CPET patient 1

CPET patient 2

CPET patient 3
Graphics 1, 2, and 3 demonstrate the lactate curves during treadmill exercise (blue) and swimming exercise (orange). Lactate values are shown on the y axis in mmol/l.

Lactate curve patient 1

Lactate curve patient 2

Lactate curve patient 3
Graphics 4, 5, and 6 show the course of heart rate, transcutaneous oxygen saturation and perfusion index during immersion, submersion and a short period thereafter. For a better display, the time axis differs between the patients. An overall stable course of oxygen saturation was seen in all three patients. In addition, the perfusion index, as a marker of peripheral vasoconstriction drops in all three patients while entering the pool. Patient number 2 did only submerse for a few seconds and was therefore asked to repeat the short apnea dive. A slight drop in heart rate while entering the pool was seen in patients 1 and 2, while the atrial arrhythmia in patient 3 made the interpretation impossible.

Immersion and diving response patient 1

Immersion and diving response patient 2

Immersion and diving response patient 3
Patient 1:
Figure 1
Graphic 1 shows the lactate curves during exercise
Graphic 4 shows the physiologic response to immersion and submersion
Patient 2:
Figure 2
Graphic 2 shows the lactate curves during exercise
Graphic 5 shows the physiologic response to immersion and submersion
Patient 3:
Figure 3
Graphic 3 shows the lactate curves during exercise
Graphic 6 shows the physiologic response to immersion and submersion
Discussion
To date, this is the first study to evaluate the basic effects of immersion and submersion on patients with Fontan physiology. Importantly, the very small number of only three patients included into this study has to be kept in mind when looking at the presented data, that has to be seen as a first insight and does not allow for any generalization.
The current study found similar physiologic reactions comparing on land and in water exercise stress testing. Heart rate response and oxygen uptake were comparable on land and in the water. At least the three patients included into this study did not suffer major adverse events triggered by immersion or submersion. To enhance a better understanding of adaptive mechanisms in Fontan patients and thereby enable interpretation of the presented data, the following rows will depict the basic mechanisms of adaption to immersion or submersion reported in healthy humans.
The basic mechanism of all immersion-associated physiologic adaptions is a redistribution of blood to the central, oxygen-dependent organs like the heart and brain, as well as a reduction of blood flow to tissues like the skeletal muscles, more tolerant to anoxia. As has been reported by Clarke et al. [9] the normal response to head-out body immersion in healthy individuals is as follows. With rising hydrostatic pressure from the shoulders to the feet with immersion of the body, a venous compression and volume translocation of 500 to 1000 ml blood volume toward the thorax is initiated [10]. Central venous pressure rises and cardiac chambers dilate in dependency of tissue compliance. Cardiac output increases by around 30% mainly through exaggerated stroke volume, while heart rate will drop in average about 6% [11, 12]. A small increase in arterial blood pressure that is, like the heart rate drop, mainly dependent on water temperature, has been reported [10, 13]. Pulmonary artery pressure will increase from 4 to 16 mmHg, as well as pulmonary wedge pressure will rise [14]. Lung volumes will be decreased, including RV, ERV, FRC, and TLC [15]. Colder water seems to further reduce vital capacity, possibly caused by increased vasoconstriction causing a greater central blood shift [16].
The normal breath-hold diving response resembles the response to head-out body immersion while adding additional influences including face immersion, hypoxia and hypercapnia. Facial immersion is the most powerful trigger for sinus bradycardia that typically occurs within 10 s of submersion, while minimum heart rates are seen at around 30 to 60 s of diving [17]. Several reports separate apnea and cold bradycardia. Lower water temperatures are inversely proportional to the extent of bradycardia. The bradycardia induced by mere face immersion is counteracted by a tachycardia during body immersion. While the first mechanism is thought to be an evolutionary remnant of mammalian reflexes, the latter one is thought to be an arousal reaction in expectation of a dive [18]. Both reflexes are transient and will only occur for the first minutes during a classic scuba dive.
The Fontan procedure or modified Fontan procedure like the total cavopulmonary connection (TCPC) is a method used for surgical palliation of a wide range of functional single ventricle congenital heart defects [19, 20]. It is associated with a good quality of life and enables patients to reach even older adulthood [21]. Although nearly all of these patients suffer from a more or less pronounced congestive heart failure most patients show only moderately reduced physical capacity. With the development of surgical technique and henceforth excellent long-term survival, cardiovascular risk factors and an active and healthy lifestyle are becoming more of an issue for long-term perseverance of quality of life and health [22, 23]. In this regard, swimming displays excellent recreational activity. In addition, the ability to swim plays a major role in the prevention of drowning in the western world. Despite various underlying anatomical variations, the main physiologic common feature is the absence of a pre-pulmonary ventricle. In contrast to a normal heart, these patients lack a contractile chamber that actively pumps blood through the lungs. There is only passive pulmonary blood flow mainly driven by inspiratory negative intrathoracic pressure. Pulmonary blood flow and cardiac output are dependent on pulmonary vascular resistance, intrathoracic pressure, central venous pressure and left atrial pressure.
With this in mind, many physicians restrict patients after Fontan procedure from swimming and particularly breath-hold diving [4]. In theory, these patients might be at risk for adverse events. Baseline worries are acute hemodynamic failure with the initial volume shift, resulting in an increased preload in the absence of a contractile pre-pulmonary chamber and the additional increase in afterload by vasoconstriction in the presence of congestive heart failure. It has been hypothesized that patients may suffer from acute pump failure or fainting due to low cardiac output. Furthermore, it has been speculated that the less negative intrathoracic pressure in the context of an increased pulmonary arterial pressure may provide a further risk for low cardiac output.
When looking at the presented data, it remains important to recognize that due to the low number of patients and heterogenous anatomy, the current data do not allow for a statistical analysis or uncritical generalization of the findings. The data rather have to be seen as a first insight, with some baseline findings that may help to plan and conduct further studies.
Following, the authors took a closer look at the effects of immersion, given by the collected data. First of all, there were no adverse events triggered by swimming. This was one of the major concerns when not only exposing Fontan patients to immersion but also performing a vigorous exercise during immersion. The latter can be seen as a provocative maneuver to see the effects of immersion even under intense circulatory demands. For safety reasons patients were not obliged to reach the same level of full exertion during the swimming exercise test as was done during the treadmill testing. This can be seen in substantial differences in the maximum RER reached, comparing both test settings. As no meaningful \(\dot{V}O_{{2{\text{peak}}}}\) \(\dot{V}{O}_{2peak}\) was reached during the swimming test, comparisons between treadmill and swimming exercise should focus on the measurements at the ventilatory threshold (VT1). The VT1 should represent a similar degree of cardiopulmonary workload independent from the test setting. As the main question was if swimming as an exercise might put Fontan patients at risk for severe adverse events, it is worth mentioning that the degree of exertion reached at VT1 during the actual swimming test, was probably still be slightly above the level of exertion that would be reached during a recreational swim. This assumption is supported by the lactate values reached during the swimming and the treadmill exercise testing, that still underline vigorous athletic activity in both tests. As a result, the measurements and physiologic reactions recorded at VT1 will probably be of clinical value as they reflect at least the degree of exertion reached by patients during swimming as a leisure activity.
When looking at the graphs, it has to be mentioned that patient 3 suffered from ectopic atrial tachycardia both during the treadmill as well as swimming exercise. The arrhythmia was known from the patients history. As the patient was motivated to finish both tests, we could include her into the study. Yet, it can be seen from the exercise, as well as diving response testing, that the tachycardia did severely compromise the patient´s performance and interpretation of her data. It might be speculated that the earlier occurrence of ectopic atrial tachycardia during the swimming stress test after 2 min, in comparison to the occurrence after 8 min during treadmill stress testing might hint at an earlier increase in atrial filling pressures and thereby triggering of the arrhythmia during the swimming stress test.
Now, comparing the graphs of treadmill and swimming exercise a comparable reaction to increasing workload can be seen. Both types of exercise lead to a linear increase of \(\dot{V}O_{2}\) and \(\dot{V}CO_{2}\).
Heart rate incline at the beginning of the swimming stress test seems to be a little steeper than during treadmill stress testing. This might simply be because the test setting in the counter current pool was a bit more irritating and it was more complicate to find an optimal counter current water speed that allowed for easy accommodation to the stress test. Another explanation might be that the first volume shift to the heart and lungs during immersion, and with beginning exercise might be compensated with a higher heart rate. This might be needed as the compliance of univentricular hearts to deal with the increased volume will be lower than in a two-chambered heart, especially in the presence of mild to moderate congestive heart failure.
All patients showed a reduced O2 pulse as an expression of congestive heart failure, yet, there is no difference seen in O2 pulse between swimming and treadmill exercise at VT1. Despite the lack of a pre-pulmonary chamber the effects of immersion in the test setting seemed to be sufficiently compensated in all three patients to prevent severe hemodynamic failure.
With regard to breathing parameters during stress, depicted in the Wassermann table 7 (\(VT/\dot{V}E\)), there is a similar slope comparing treadmill and swimming exercise. Only under severe workload there seems to be a little bit more scattering of the breathing graphs, possibly indicating a rather ineffective breathing pattern or a lower respiratory capacity due to decreased lung volumes during immersion. Yet, despite the artificial setup with a snorkel connected to a spirometry face mask and the strenuous swimming exercise, it can be recognized that even this rather uncoordinated breathing pattern did not lead to immediate cessation of the swimming exercise, as could have been expected when thinking about a possible circulatory compromise due to not using the negative intrathoracic pressure effectively for lung perfusion in these patients.
When moving further to the effects of submersion, the graphical data of immersion and short submersion on the physiologic parameters tcO2, heart rate, and the perfusion index should be evaluated.
All three patients showed stable tcO2 throughout the testing period. The effect of immersion can be seen clearly in a drop of the perfusion index indicating peripheral vasoconstriction as part of the initial redistribution of blood volume as described above. In this context, data imply that Fontan patients have to deal with a similar volume shift due to peripheral vasoconstriction as has been reported in healthy human subjects [11, 12]. Similar to reports in healthy subjects, the heart rate drop with immersion can be seen, while the effect is only mild. As all three patients accomplished only very short diving times of under 10 s data cannot adequately indicate if there might be a major heart rate drop during submersion, as the main diving bradycardia is reported to occur after 10 s with a maximum at about 30 to 60 s of diving. In fact, during this very short dive, two of three patients showed an increase in heart rate. As has been stated above, heart rates in patient 3 are hard to interpret as she suffered from ectopic atrial tachycardia (EAT). During the immersion and submersion testing period she had an EAT with 2:1 to 3:1 conduction, making it impossible to interpret heart rate response in patient 3. After all, it has to be mentioned that the physiologic responses reported in this study are recorded under artificial circumstances. Especially the relatively high surrounding temperature of about 32 °C in the pool area and a relatively high water temperature of 28° degrees Celsius could be important when looking at the extent of the reported effects. It can only be speculated that lower temperatures might influence the reported findings.
Conclusion
This study presents the first-in-man data on swimming and diving in Fontan patients. Basically, the physiologic response to exercise was comparable on land and in the water. While data on breath-hold diving are insufficient to enable a conclusion, the physiological data of the three tested patients showed a similar response to a swimming exercise as has been reported in healthy subjects. Importantly, this study included only three patients and larger studies are needed to evaluate the reported findings!
Limitations
The main limitation of this study is the small number of patients as well as the none blinded study protocol that had to be chosen for optimal patient safety in view of possible adverse events. The swimming stress test was not performed until complete exhaustion due to safety reasons. In addition, a possibly substantial selection bias has to be reported as there were only Fontan patients included who stated that they are familiar with swimming and diving.
References
Lazar JM, Khanna N, Chesler R, Salciccioli L (2013) Swimming and the heart. Int J Cardiol 168(1):19–26
Epstein M (1978) Renal effects of head-out water immersion in man; implications for understanding of volume homeostasis. Physiol Rev 58:529
Lehmann M, Samek L (1990) Recreational swimming in CHD patients and healthy control subjects in relation to left heart function. Clin Cardiol 13(8):547–554
Lotshaw AM, Thompson M, Sadowsky S, Hart MK, Millard MW (2007) Quality of life and physical performance in land- and water-based pulmonary rehabilitation. J Cardiopulm Rehabil Prev 27:247–251
Shah P, Pellicori P, Macnamara A, Urbinati A, Clark AL (2017) Is swimming safe in heart failure? A systematic review. Cardiol Rev 25(6):321–325
Asplund CA, Creswell LL (2016) Hypothesised mechanisms of swimming-related death: a systematic review. Br J Sports Med 50(22):1360–1366
Pelliccia A et al (2020) ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. The Task Force on sports cardiology and exercise in patients with cardiovascular disease of the European Society of Cardiology (ESC). Eur Heart J. https://doi.org/10.1093/eurheartj/ehaa605
Aadland E, Solbraa AK, Resaland GK, Steene-Johannessen J, Edvardsen E, Hansen BH, Anderssen SA (2017) Reference values for and cross-validation of time to exhaustion on a modified Balke protocol in Norwegian men and women. Scand J Med Sci Sports 27(11):1248–1257
Fitz-Clarke JR (2018) Breath-hold diving. Compr Physiol 8(2):585–630
Arborelius M, Bllidin UI, Lilja B, Lundgren CE (1972) Hemodynamic changes in man during immersion with the head above water. Aerosp Med 43:592–598
Park KS, Chois JK, Park YS (1999) Cardiovascular regulation during water immersion. Appl Human Sci 18:233–241
Lin YC (1984) Circulatory functions during immersion and breathhold dives in humans. Unsersea Biomed Res 11:123–138
Campbell LB, Gooden BA, Horowitz JD (1969) Cardiovascular response to partial and total immersion in man. J Phyiol (Lond) 202:239–250
Lollgen SH, von Nieding G, Koppenhagen K, Kerstin F, Just H (1981) Hemodynamic response to graded water immersion. Klin Wochenschrift 59:623–628
Rahn H, Otis AB, Chadwick LE, Fenn WO (1946) The pressure volume diagram of the thorax and lung. Am J Physiol 146:161–178
Kurss DI, Lundgren CEG, Pasche AJ (1971) Effects of water temperature on vital capacity in headout immersion. In: Bachrach AJ, Matzgen MM (eds) Underwater physiology VII. Undersea Medical Society, Bethesda, MD, pp 297–301
Yamaguchi H, Tanaka H, Obara S, Tanabe S, Utsuyama N, Takahashi A, Nekahira J, Yamamoto Y, Jiang ZL, He J (1993) Changes in cardiac rhythm in man during underwater subermsion and swimming studied by ECG telemetry. Eur J Appl Physiol 66:43–48
Speck DF, Bruce DS (1978) Effects of varying thermal and apneic conditions on the human diving reflex. Undersea Biomed Res 5:9–14
Arunamata A, Tacy TA, Kache S, Mainwaring RD, Ma M, Maeda K, Punn R (2020) Recent outcomes of the extracardiac Fontan procedure in patients with hypoplastic left heart syndrome. Ann Pediatr Cardiol 13(3):186–193
Stellin G (2020) A Tribute to the pioneers of right heart bypass: an historical review. World J Pediatr Congenit Heart Surg 11(2):198–203
Bucholz EM, Sleeper LA, Goldberg CS, Pasquali SK, Anderson BR, Gaynor JW, Cnota JF, Newburger JW (2020) Socioeconomic Status and long-term outcomes in single ventricle heart disease. Pediatrics 146(4):e20201240
Scheffers LE, Berg LEV, Ismailova G, Dulfer K, Takkenberg JJ, Helbing WA (2020) Physical exercise training in patients with a Fontan circulation: a systematic review. Eur J Prev Cardiol. https://doi.org/10.1177/2047487320942869
Holbein CE, Veldtman GR, Moons P, Kovacs AH, Luyckx K, Apers S, Chidambarathanu S, Soufi A, Eriksen K, Jackson JL, Enomoto J, Fernandes SM, Johansson B, Alday L, Dellborg M, Berghammer M, Menahem S, Caruana M, Kutty S, Mackie AS, Thomet C, Budts W, White K, Sluman MA, Callus E, Cook SC, Khairy P, Cedars A (2019) Perceived health mediates effects of physical activity on quality of life in patients with a fontan circulation APPROACH-IS consortium and the International Society for Adult Congenital Heart Disease (ISACHD). Am J Cardiol 124(1):144–150
Disclosure
The authors have no financial relationships relevant to this article to disclose.
Funding
The current study was funded by the Kinderherzkammer Leipzig e.V.. The study was supported by CORTEX Biophysik GmbH.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare to have no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and / or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study received ethical approval by the ethics committee University of Leipzig and is listed under the reference 549/19-ek.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Paech, C., Gebauer, R.A., Weidenbach, M. et al. The Fontan and the Sea: First-in-Man Data on Swimming and Diving Physiology in Fontan Patients. Pediatr Cardiol 42, 1614–1624 (2021). https://doi.org/10.1007/s00246-021-02649-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-021-02649-3