
Abstract
Pediatric cardiac surgery with cardiopulmonary bypass (CPB) induces a complex inflammatory response that may cause multiorgan dysfunction. The objective of this study was to measure postoperative cytokine production and correlate the magnitude of this response with intraoperative variables and postoperative outcomes. Serum samples from 20 children (median age, 15 months) undergoing cardiac surgery with CPB were obtained preoperatively and on postoperative days (POD) 1–3. Serum levels of interleukin (IL)-6, IL-8, and IL-10 increased significantly on POD 1 (p < 0.01) vs pre-op values to 271 ± 68, 44 ± 9, 7.5 ± 0.8 pg/ml, respectively, whereas serum IL-1β, IL-12, and tumor neurosis factor -α were not significantly changed. The serum IL-6 and IL-8 levels correlated positively (p < 0.01) with the degree of postoperative medical intervention as measured by the Therapeutic Interventional Scoring System and indicated a greater need for inotropic support (p = 0.057). A negative correlation (p < 0.01) between IL-6, IL-8, and mixed venous oxygen saturation suggested compromised cardiopulmonary function. Patients with single ventricle anatomy had the highest levels of IL-6 and IL-8 (629 ± 131 and 70 ± 17 pg/ml, respectively), with a mean CPB time of 106 ± 23 minutes. Thus, the proinflammatory response after surgery with CPB was associated with postoperative morbidity with increased need for medical intervention.
Similar content being viewed by others

Introduction
Pediatric patients who undergo heart surgery involving cardiopulmonary bypass (CPB) are at risk of developing inflammatory complications that can result in multisystem organ dysfunction [5, 6, 7]. Several factors can trigger the postoperative systemic inflammatory response including surgical trauma, ischemia–reperfusion injury, endotoxemia, and activation of leukocytes by artificial surfaces, [20, 33]. This inflammatory process involves the activation of lymphocytes, monocytes/macrophages, endothelial cells, and cardiac myocytes that can express and secrete many proinflammatory cytokines, including tumor necrosis factor (TNF-α), interleukins (IL-1 , IL-6, and IL-8), as well as antiinflammatory cytokines IL-4, IL-10, and transforming growth factor (TGF-β) [14, 16, 17, 29, 34]. These biologically active factors have been implicated in the complications after cardiac surgery, including pulmonary dysfunction, depressed cardiac contractile activity and impaired hypothalamic–pituitary–thyroid axis [9–11, 13, 26, 31].
Global myocardial ischemia followed by reperfusion injury may result during surgery involving CPB with aortic cross-clamping. Jansen and colleagues reported that TNF-α could be detected after release of the aortic cross-clamp, and that the duration of aortic cross-lamp was an independent predictor of postoperative serum TNF-α and IL-6 levels [21]. Furthermore, myocardial production and release of biologically active TNF-α and IL-8 may be involved in the postischemic myocardial depression or “stunning” after CPB [4, 11, 22, 27, 34). Complement activation and cytokine production have also been reported in cardiac surgery performed without the aid of cardiopulmonary bypass [32].
The antiinflammatory cytokine IL-10 is also released during CPB and has been shown to either directly inhibit the release of proinflammatory cytokines [12, 14] or exert antiinflammatory effects by triggering the release of IL-1 receptor antagonist and TNF soluble receptors 1 and 2 [25].
Several therapeutic strategies have been proposed that aim to modulate the inflammatory response in this clinical setting, including hemofiltration [2, 30], use of steroids and nonsteroidal antiinflammatory agents [3, 15, 24], and complement receptor blocking agents [8]. Ultrafiltration procedures have been widely adopted and shown to be effective in attenuating the inflammatory response, resulting in improved postoperative hemodynamics, decreased duration of mechanical ventilator support, and decreased length of stay in intensive care unit [2, 30]. Treatment of adults undergoing heart surgery with cardiopulmonary bypass with methylprednisolone has yielded promising results showing reduced production of proinflammatory cytokines, TNF-α, IL-6, and IL-8 and increased IL-10 [24, 32]. However, administration of steroids to pediatric patients undergoing CPB has not been shown to suppress the inflammatory reaction, nor has it improved postoperative outcome measures [15]. Thus, novel therapeutic targets and approaches are still necessary to minimize the systemic inflammatory response in children undergoing cardiac surgery.
The objective of this study was to measure the cytokine response in the postoperative period and correlate these results with intraoperative variables and postoperative outcomes.
Materials and Methods
The study protocol was approved by the institute’s committee on human rights in research. Informed consent was obtained from either parent(s) or guardian(s) before the operation, and patients older than 7 years of age gave consent. Twenty children of either gender younger than age 18 years who were subject to surgical correction of congenital heart defects with CPB were recruited into the study. The median age, gender, and specific anatomic defects of these patients are listed in Table 1.
Surgery and Anesthesia
Operations were performed by one cardiothoracic surgeon, and conventional general anesthesia was used in all patients. Endotracheal intubation and placement of central venous and arterial catheters were performed after induction of anesthesia. Antibiotic prophylaxis was given at the induction of anesthesia and at the end of the surgical procedure. Heparinization was achieved with heparin sulfate, and its effect was reversed using protamine sulfate. Aprotinin was administered to all patients, performed with aortic and venous cannulation, membrane oxygenation, and nonpulsatile flow. Similar techniques to maintain hematocrit and pH were used in all patients. If necessary at the end of the surgical procedure intracardiac catheters (left and right atria) were placed for postoperative care. Patients received standard care in the postoperative period in the pediatric intensive care unit. Corticosteroids were not administered.
Postoperative Management and Measures of Clinical Outcome
Patients were continuously monitored in the intensive care unit. Data on clinical outcomes, including quantities of vasodilator and inotropic drugs, blood gas and lactate analyses, urine output, blood pressures, cardiac rhythm, and heart rates, were recorded daily. Mixed venous oxygen saturation (MVSat) (%) of blood samples obtained from the superior vena cava or pulmonary artery (when accessible) was determined by standard blood gas analysis. The degree of inotropic support required was calculated as described by Wernovsky et al. [35]. The overall degree of postoperative care was analyzed by calculating the Therapeutic Interventional Scoring System (TISS). TISS scores were derived daily for 76 different therapeutic and monitoring procedures and reflected the invasiveness, intensity, and complexity of care rendered to the patient.
Cytokine Analysis
Blood samples for cytokine analysis were collected after induction of anesthesia and before institution of CPB, and on postoperative days (POD) 1–3. One milliliter of blood was collected in a heparinized tube and the serum separated by centrifugation (5000g for 10 minutes at 4°C) and stored at −20°C until analyzed.
TNF-α and IL-1β, IL-12, IL-6, IL-8, and IL-10 were measure’d by means of two commercially available kits, the Human Th1/Th2 and Human Inflammatory Cytokine Bead Array (BD Biosciences Pharmingen, San Jose, CA, USA). The Cytokine Bead Array system generates data that are comparable to enzyme-linked immunosorbant assays but in a “multiplexed” or simultaneous fashion employing a series of particles with discrete fluorescence intensities to simultaneously detect multiple soluble analytes. The concentration of unknowns is calculated for the cytometric bead array through the use of known standards and plotting unknowns against a standard curve.
Statistical Analysis
Results are expressed as median (ranges) or mean ± SE. Analysis of the data at different time points was performed using one-way repeated measures analysis of variance (ANOVA) and pairwise multiple comparison procedures by the Holm–Sidak method. Strength of association between cytokines and clinical measures were assessed by Pearson product moment correlation test. A p value < 0.05 was considered significant. Data were analyzed using SigmaStat statistical software, version 3.1 (Systat Software, Richmond, CA, USA).
Results
Table 1 shows the types of congenital heart disease and the number in each category. The median age was 15 months (range 0.1–180), with equal gender distribution. The mean duration of CPB was 106 ± 44 minutes (n = 20 patients), and the mean aortic cross-clamp time was 69 ± 40 minutes (n = 18 patients). Postoperative outcome measures are listed as median values and ranges. The TISS and inotropic score for each patient represent the sum of the scores on POD 1–3. MVsat (%) and blood lactate (mmol/L) levels are those measured on POD 1.
Inflammatory Response to CPB
Figure 1 shows the serum levels of proinflammatory cytokines IL-6 and IL-8 and the inflammatory cytokine IL-10 following corrective heart surgery. Concentrations of all three cytokines were significantly elevated on POD 1 compared to their preoperative values. POD 1 serum IL-6 and IL-8 values were 271 ± 68 and 44 ± 9 pg/ml (mean ± SE), respectively, compared with preoperative values of 46 ± 12 and 16 ± 2 pg/ml, respectively. All three cytokines declined on POD 2 and 3 and were not significantly different from their preoperative values. Serum IL-6 levels correlated positively with IL-8, with a statistically significant (p < 0.001) correlation coefficient (r 2) of 0.7742. Intraoperative variables, including cardiopulmonary bypass time and aortic cross-clamp time, did not significantly correlate with the maximum postoperative serum IL-6 and IL-8 response (data not shown).

Systemic inflammatory response after CPB. Serum concentrations of IL-6, IL-8, and IL-10 were measured preoperatively and on postoperative day (POD) 1–3. Twenty patients underwent cardiopulmonary bypass surgery; n = 20 on pre- and POD 1, n = 13 on POD 2 and n = 8 on POD3. The horizontal line is the median value; the box encompasses 25th to 75th percentiles, and caps represent 10 and 90%. *p < 0.01 vs preoperative value; **p < 0.01 vs mean values at all other time points. Statistical significance was determined by repeated measures ANOVA with pairwise multiple comparison procedure (Holm–Sidak method)
Patients with single ventricle anatomy had the highest serum IL-6 and IL-8 levels on POD 1, with mean ± SE values of 629 ± 131 and 70 ± 17, respectively, and a mean CPB time of 106 ± 23 minutes. Six of eight cyanotic patients had maximum serum IL-6 values > 100 pg/ml, whereas only 3 of 12 noncyanotic patients had these high values.
Table 2 summarizes the serum concentrations of TNF-α, IL-1β, and IL-12 measured pre- and post-CBP. Although serum TNF-α and IL-12 increased by POD2 these increases did not reach statistical significance.
Correlations of Clinical Outcomes with Cytokine Responses
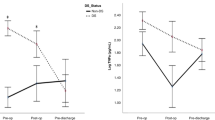
The postoperative outcomes that were examined are listed in Table 1. No significant correlation was found between the maximum cytokine (IL-6, and IL-8 on POD 1) response and total time in the intensive care unit, length of hospital stay, and days of mechanical ventilation. However, serum IL-8 concentrations on POD 1 correlated negatively with MVsat, an indicator of decreased oxygen delivery to the peripheral tissue, and positively with cumulative TISS scores on POD 1–3. These correlations reached a level of significance of p = 0.009, as shown in Fig. 2. Higher IL-8 levels also correlated with higher inotropic scores on POD 1 (p = 0.057), whereas no correlation was found with blood lactate values (Table 3). Similar correlations were found between the maximum serum IL-6 response and these clinical outcome measures, as shown in Table 3.

Cytokine response correlates with postoperative outcomes. On postoperative day (POD) 1, patient mixed venous oxygen saturation (MV sat , %) values show significant negative correlation with serum IL-8 levels (p < 0. 009). Cumulative TISS scores from POD 1–3 correlate significantly with serum IL-8 levels (p < 0.009). The line represents the best fit linear regression curve. Significance of the correlation coefficient was determined by ANOVA
Discussion
In this study, we showed a significant positive correlation between the magnitude of the inflammatory response as measured by serum concentrations of IL-6 and IL-8 after CPB surgery and the degree of medical intervention (TISS and inotropic score) of the pediatric patient in the early postoperative period. Higher TISS scores with a greater proinflammatory response reflected an increase in postoperative management requirements. Similarly, the need for inotropic support was greater in patients with higher postoperative serurn IL-8 levels. MVsat was 34–78% on POD 1, and these values correlated negatively with serum IL-8 concentrations, further supporting the hypothesis that the magnitude of the inflammatory response has a direct effect on oxygen delivery to the peripheral tissues and postoperative morbidity of the pediatric patient. This inflammatory response was observed despite the routine use of modified ultrafiltration procedures and aprotinin in our surgical practice to reduce circulating cytokines and complement factors, and to increase hemoglobin, hematocrit, and platelet levels, as has been reported by others [2, 18, 28, 30]. Our data support a recent study showing significant correlations of postoperative serum IL-6 and IL-8 with increased inotropic requirements and reduced arterial oxygen tension (PaO2) 2 hours after CPB [16]. In addition, these authors found that the cytokine response correlated positively with length of mechanical ventilation post-surgery which we did not observe. In contrast to other studies [20], we did not find a correlation between postoperative serum cytokines and the duration of CPB or aortic cross-clamp, possibly due to the diverse nature of the surgical procedures. However, we did observe higher serum proinflammatory cytokines postoperatively in six of eight cyanotic patients in whom the duration of CPB was > 90 minutes. Furthermore, all patients with single ventricle anatomy had the highest levels of IL-6 and IL-8 (629 ± 131 and 70 ± 17 pg/ml, respectively), with a mean CPB time of 106 ± 23 minutes. One patient (with double ventricle anatomy) with bronchomalacia had the highest postoperative serum IL-6 and IL-8 concentrations (888 and 132 pg/ml, respectively), with a CPB time of 145 minutes and a complex postoperative course. Taken together, these data support the hypothesis that the duration of CPB, the complexity of anatomical defect and surgical repair, and the presence of cyanosis are contributing factors to the postoperative inflammatory response.
Results from a recent study that tested the efficacy of corticosteroid treatment to reduce the inflammatory response in pediatric cardiac surgery patients were negative, with no effect on postoperative recovery [15]. Steroid pretreatment remains controversial because steroids may inhibit TNF-α, IL-6, and IL-8 production, thus preventing peripheral vasodilatation, but they may also increase the release of endotoxin [1, 3]. Thus, the search for novel therapeutic targets is warranted in this clinical setting. The identification of other mediators of inflammation, including macrophage migration inhibitory factor and HMGB1 (high mobility group box-1 protein), as well as a focus on pulmonary-derived cytokines may provide another strategy in the treatment of postoperative inflammation in the heart surgery patient [10, 23]. Since pulmonary injury and multiorgan dysfunction remain significant complications following cardiac surgery, continued efforts to identify the mediators of these effects are required to potentially reduce postoperative morbidity in the pediatric patient.
References
Andersen LW, Baek L, Thomsen BS, Rasmussen JP (1989) Effect of methylprednisone on endotoxemia and complement activation during cardiac surgery. J CardioThorac Anesth 3:544–549
Berdat PA, Eichenberger E, Ebell J, et al. (2004) Elimination of proinflammatory cytokines in pediatric cardiac surgery: analysis of ultrafiltration method and filter type. J Thorac Cardiovasc Surg 127:1688–1696
Bourbon A, Vionnet M, Leprince P, et al. (2004) The effect of methylprednisolone treatment on the cardiopulmonary bypass-induced systemic inflammatory response. Eur J Cardiothorac Surg 26:932–938
Burns SA, Newburger JW, Xiao M, et al. (1995) Induction of interleukin-8 messenger RNA in heart and skeletal muscle during pediatric cardiopulmonary bypass. Circulation 92(Suppl):315–321
Butler J, Pathi VL, Paton RD, et al. (1996) Acute-phase responses to cardiopulmonary bypass in children weighing less than 10 kilograms. Ann Thorac Surg 62:538–542
Casey LC (1993) Role of cytokines in the pathogenesis of cardio-pulmonary-induced multisystem organ failure. Ann Thorac Sura 56:S92–S96
Casey WF, Hauser GJ, Hannallah RS, Midgley FM, Khan WN (1992) Circulating endotoxin and tumor necrosis factor during pediatric cardiac surgery. Crit Care Med 20:1090–1096
Chai PJ, Nassar R, Oakeley AE, et al. (2000) Soluble complement receptor-1 protects heart, lung and cardiac myofilament function from cardiopulmonary bypass damage. Circulation 101:541–546
Chowdhury D, Ojamaa K, Parnell VA, et al. (2001) A prospective randomized clinical study of thyroid hormone treatment after operations for complex congenital heart disease. J Thorac Cardiovasc Surg 12:1023–1025
de Mendonca-Filho HT, Gomes RV, de Almeida Campos LA, et al. (2004) Circulating levels of macrophage migration inhibitory factor are associated with mild pulmonary dysfunction after cardiopulmonary bypass. Shock 22:533–537
Finkel MS, Oddis CV, Jacob TD, et al. (1992) Negative inotropic effects of cytokines on the heart mediated by nitric oxide. Science 257:387–389
Fiorentino DF, Zlotnik A, Mosmann TR, Howard M, O’ Garra A (1991) IL-10 inhibits cytokine prodution by activated macrophages, J Immunol 147:3815–3822
Gando S, Nishihira J, Kemmotsu O, et al. (2000) An increase in macrophage migration inhibitory factor release in patients with cardiopulmonary bypass surgery. Surg Today 30:689–694
Gerard C, Bruyns C, Marchant A, et al. (1993) lnterleukin-10 reduces the release of tumor necrosis factor and prevents lethality in experimental endotoxemia. J Exp Med 177:547–550
Gessler P, Hohl V, Carrel T, et al. (2005) Administration of steroids in pediatric cardiac surgery: impact on clinical outcome and systemic inflammatory response. Pediatr Cardiol 26:595–600
Gessler P, Pfenninger J, Pfammatter JP, et al. (2003) Plasma levels of interleukin-8 and expression of interleukin-8 receptors on circulating neutrophils and monocytes after cardiopulmonary bypass in children. J.Thorac Cardiovasc Surg 126:718–725
Gessler P, Pretre R, Hohl V, et al. (2004) CXC-chemokine stimulation of neutrophils correlates with plasma levels of myeloperoxidase and lactoferrin and contributes to clinical outcome after pediatric cardiac surgery. Shock 22:513–520
Greilich PE, Brouse CF, Whittem CW, et al. (2003) Antifibrinolytic therapy during cardiopulmonary bypass reduces proinflammatory cytokine levels: a randomized, double-blind, placebo-controlled study of epsilon-aminocaproic acid and aprotinin. J Thorac Cardiovasc Surg 126:1498–1603
Hennein HA, Ebba H, Rodriguez JL, et al. (1994) Relationship of the proinflammatory cytokines to myocardial ischemia and dysfunction after uncomplicated coronary revascularization. J Thorac Cardiovasc Surg 108:626–635
Hirai S (2003) Systemic inflammatory response syndrome after cardiac surgery under cardiopulmonary bypass. Ann Thorac Cardiovasc Surg 9:365–370
Jansen NJG, van Orveren W, van der Broek L, et al. (1991) Inhibition by dexamethasone of the repefusion phenomena in cardiopulmonary bypass. J Thorac Cardiovasc Surg 102:515–525
Kapadia S, Lee J, Torre-Amine G, et al. (1995) Tumor necrosis factor-α gene and protein expression in adult feline myocardium after endotoxin administration. J Clin Invest 96:1042–1052
Lin X, Yang H, Sakuragi T, et al. (2005) Alpha-chemokine receptor blockade reduces high mobility group box1 (HMGB1) protein induced lung inflammation and injury and improves survival in sepsis. Am J Physiol Lung Cell Mol Physiol 289:583–590
McBride WT, Allen S, Gormley SM, et al. (2004) Methylprednisolone favourably alters plasma and urinary cytokine homeostasis and subclinical renal injury at cardiac surgery. Cytokine 27:81–89
McBride WT, Armstrong MA, Crockard AD, McMurray TJ, Rea JM (1995) Cytokine balance and immunosuppresive changes at cardiac surgery: contrasting response between patients and isolated CPB circuits. Br J Anaesth 75:724–733
McMahon CK, Klein I, Ojamaa K (2003) lnterleukin-6 and thyroid hormone metabolism in pediatric cardiac surgery patients. Thyroid 13:301–304
Metinko AP, Kunkel SL, Standiford TJ, et al. (1992) Anoxia–hyperoxia induces monocyte-derived interleukin-8. J Clin Invest 90:791–798
Millar AB, Armstrong L, van der Linden J, et al. (1993) Cytokine production and hemofiltration in children undergoing cardiopulmonary bypass. Ann Thorac Surg 56:1499–1502
Qing M, Schumacher K, Heise R, et al. (2003) Intramyocardial synthesis of pro- and anti-inflammatory cytokines in infants with congenital cardiac defects. J Am Coll Cardiol 41:2266–2274
Sever K, Tansel T, Basaran M, et al. (2004) The benefits of continuous ultrafiltration in pediatric cardiac surgery. Scand Cardiovasc J 38:307–311
Stayer SA, Diaz LK, East DL, et al. (2004) Changes in respiratory mechanics among infants undergoing heart surgery. Anesth Analg J 98:49–55
Tarnok A, Hambsch J, Emmrich F, et al. (1999) Complement activation, cytokines, and adhesion molecules in children undergoing cardiac surgery with or without cardiopulmonary bypass. Pediatr Cardiol 20:113–125
Varan B, Tokel K, Mercan S, Donmez A, Aslamaci S (2002) Systemic inflammatory response related to cardiopulmonary bypass and its modification by methyl prednisolone; high dose versus low dose. Pediatr cardiol 23:437–441
Wan S, DeSmet JM, Barvais L, et al. (1996) Myocardium is a major source of proinflammatory cytokines inpatients undergoing cardiopulmonary bypass. J Thorac Cardiovasc Surg 112:806–811
Wernovsky G, Wypij D, Jonas RA, et al. (1995) Postoperative course and hemodynamic profile after the arterial switch operation in neonates and infants: a comparison of low-flow cardiopulmonary bypass and circulatory arrest. Circulation 92:2226–2235
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Madhok, A.B., Ojamaa, K., Haridas, V. et al. Cytokine Response in Children Undergoing Surgery for Congenital Heart Disease. Pediatr Cardiol 27, 408–413 (2006). https://doi.org/10.1007/s00246-006-0934-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-006-0934-y