
Abstract
Purpose
Statin-induced myopathy (SIM) is the commonest reason for discontinuation of statin therapy. The aim of this present meta-analysis is to assess the relationship between glycine amidinotransferase gene (GATM) polymorphism and risk of SIM.
Methods
MEDLINE, EMBASE, Web of Science, and Cochrane Library databases were searched systematically for case-control studies investigating the relationship between GATM polymorphism and SIM. Retrieved articles were carefully reviewed and assessed according to the inclusion criteria. Associations were assessed in pooled data by calculating odds ratio with 95% confidence intervals. Subgroup analysis was performed according to comedications and severity of SIM.
Results
Six studies with 707 cases and 2321 controls were included in this meta-analysis. GATM rs9806699 G>A was associated with decreased risk of SIM (OR = 0.80, 95% CI 0.68–0.94, P = 0.006). This association remained significant in the subgroup with fibrates or niacin excluded. However, the association of rs9806699 G>A with severe SIM was not significant. In addition, another two variations at GATM, rs1719247 C>T, and rs1346268 T>C were also associated with declined risk of SIM.
Conclusions
GATM polymorphism including rs9806699 G>A, rs1719247 C>T, and rs1346268 T>C may be protective factors of SIM. GATM rs9806699 G>A may only exert protective effect on mild SIM cases. Our meta-analysis indicates that GATM polymorphism may represent a pharmacogenomics biomarker for predicting incidence of SIM, which contributes to risk stratification and optimizing statin adherence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Statin-induced myopathy (SIM) is the most frequently reported adverse effect of statins and is the commonest cause for discontinuation of statin therapy [1]. Symptoms of SIM can vary from mild myalgia to rare but life-threatening rhabdomyolysis [2]. The high prevalence of statin use made the absolute number of SIM became more substantial. Unfortunately, the underlying mechanisms of SIM have not been fully understood. Risk factors of SIM have been investigated in the past, such as high statin doses, older age, hypothyroidism, hepatic, and renal insufficiency [3,4,5]. Recently, genetic predisposition was found to play a crucial role in SIM [6]. It is now well established that a single nucleotide polymorphism (SNP) of solute carrier organic anion transporter family member 1B1 (SLCO1B1), rs4149056 T > C, increases the risk of SIM [7]. The association of SNPs in other genes, including glycine amidinotransferase gene (GATM) and risk of SIM, has also aroused researcher’s interest.
GATM is located on chromosome 15q15.3 and it encodes a mitochondrial enzyme, L-arginine, glycine amidinotransferase (AGAT), which is a rate-limiting enzyme involved in the biosynthesis of creatine [8]. Creatine is transported to muscle tissues after synthesis in the liver and kidneys, then it is further transformed to creatine phosphate, which is participated in rapid re-synthesis of ATP [9]. It plays a pivotal role in the myocellular energy metabolism. In 2003, Mangravite et al. firstly reported the protective effect of the GATM rs9806699 G > A polymorphism on SIM in a case-control study with SIM cases of 72 [10]. The locus rs9806699 is an expression quantitative trait locus (eQTLs) for the GATM. The A allele was associated with a decline of GATM expression, leading to decline of creatine synthesis. The reduced creatine availability might affect energy metabolism of skeletal muscle cells and thus participate in the pathogenesis of SIM [9]. However, the following researches regarding the effect of rs9806699 G > A on SIM yielded conflict results [11,12,13,14,15]. Furthermore, other two SNPs, rs1719247 and rs1346268, in GATM were found to be in linkage disequilibrium with rs9806699 [7, 10], and the effect of these two SNPs have also been investigated though the results are controversial. Therefore, the role of GATM polymorphism in SIM remains a much-debated topic to date. The aim of the present study is to perform a meta-analysis to explore the relationship between GATM polymorphism and SIM, which help to identify high-risk population for SIM and provide more individualized recommendation for statin users.
Methods
This meta-analysis was reported in accordance with the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines [16]. The MOOSE checklist could be found in the Supplementary Materials A (eTable 1).
Literature search
We searched the MEDLINE, EMBASE, Web of Science, and Cochrane Library databases through May 2020 for case-control studies investigating the relationship between GATM polymorphism and SIM, with the following search terms: statin, gene encoding glycine amidinotransferase, GATM, polymorphism, muscle symptom, myopathy, rhabdomyolysis, and myositis. If available, Medical Subject Headings (MeSH) terms were used together with the free text terms and synonyms. In addition, the reference lists of the eligible studies were screened for additional relevant studies.
Study selection
We included studies that met the following criteria: (1) case-control studies investigating statin-induced myopathy, (2) genotyping and reporting GATM polymorphism in each group, (3) sample size more than 10 patients, (4) published in English, (5) allele frequencies available from the study population. Two reviewers (M.L and F.F) independently screened the titles and abstracts of all retrieved citations to identify studies that potentially met the inclusion criteria. Thereafter, the full texts of potentially relevant studies would be obtained and independently scrutinized by two reviewers (M.L and F.F) based on the above-mentioned inclusion criteria to be finally included. Disagreements were resolved by discussing until a consensus was reached.
Data extraction
Relevant data of included studies was extracted from eligible studies using a standardized form (Supplementary Material B) by two reviewers (M.L and Y.Z) independently. The following information was extracted from each study: the first author’s name, country, sample size, publication year, type of statins used, presence of interacting medications, diagnosis criteria for SIM, GATM polymorphism data (including minor allele frequency (MAF) at different sites), validity of the genotyping method, and Hardy–Weinberg equilibrium (HWE) condition of each group. Disagreements were resolved by discussing until a consensus was reached.
Study outcome
The occurrence of SIM was studied as outcome. SIM was defined as muscle symptoms or creatine kinase levels > 3 × upper limits of normal (ULN). The diagnosis of severe SIM is according to the specific diagnosis of each included study if it is available.
Quality assessment
The Newcastle–Ottawa Scale was used to assess the quality of studies and the risk of bias [17]. Studies would be assessed with prespecified criteria in three basic domains, i.e., four stars for selection, two stars for comparability, and three stars for exposure. A score > 7 suggested a low risk of bias, a score between 5 and 7 suggested a moderate risk of bias, and a score < 5 suggested a high risk of bias. Two reviewers (M.L and Y.Z) independently performed the assessment. Disagreements regarding quality assessment were resolved by discussion.
Statistical analysis
The connection between GATM polymorphism and SIM risk was reported as odds ratio (OR) with 95% confidence interval (95% CI), based on allele contrast model. Data was pooled using either random effects model or fixed effects model according to the statistical heterogeneity between studies, which was measured by Cochran Q test and the I2 statistic. Heterogeneity between studies was defined a priori as significant when I2 statistic ≥ 50% or P value of Q test < 0.05 [18, 19]. If the effects seemed to be homogeneous, the Mantel–Haenszel fixed-effect model was utilized. Otherwise, the random-effect model was used. The risk of publication bias was evaluated by funnel plot and the asymmetry of the plot distribution indicated the presence of publication bias [20]. Planned subgroup analysis was conducted in regard to the presence or absence of interacting medications, different populations, and diagnosis criteria for SIM according to whether CK elevation was obligatory or not. We also pooled OR for the risk of severe SIM if the data was available. Sensitivity analysis was conducted by excluding individual studies that were considered possible confounders to the result. All statistical analysis was performed with STATA 14.1 software (Stata Corporation, College Station, TX, USA). It is considered to be significant if the two-tailed P value was less than 0.05. The graphic compositions were performed by R version 3.3.1 (R Core Team).
Results
Study characteristics
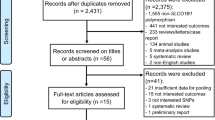
The PRISMA flow diagram of the study selection was shown in Fig. 1. We retrieved a total of 75 citations from the initial search. After removing the duplicates and screening all titles and abstracts of retrieved citations, 13 articles were further assessed by full-text review according to the above-mentioned inclusion criteria. As a result, 7 full-text articles were excluded due to the reasons shown in the Fig. 1, leaving 6 eligible studies (707 cases and 2321 controls) for final analysis. The characteristics of the included studies were summarized in Table 1. There were two independent populations in the study of Mangravite et al. [10], in which population of Marshfield was genotyped for GATM rs9806699, and population of SEARCH trial was genotyped for GATM rs1719247 and rs1346268. All of the six included studies had allelic information at rs9806699, while allelic information at rs1719247 and rs1346268 were available in the study of Floyd et al. and two independent population of Mangravite et al. Various statin treatment protocols were applied, and three of six studies excluded fibrates or niacin comedications [10, 12, 13]. The frequencies of the genotypes in three studies followed the HWE, the others were not accessible (Table 1). Three studies had data of severe SIM, and their own definitions of severe SIM were shown on Supplementary Materials A (eTable 2) [11,12,13]. The Newcastle–Ottawa Scale was used to assess the quality of included studies and the results were shown in Table 2. All the publications received more than six stars, and three of them reached eight stars, which were indicative of high quality.

PRISMA flow diagram of the study selection
Meta-analysis results
The association between GATM rs9806699 and statin-induced myopathy with subgroup analysis
The combined data from six eligible case-control studies proved that GATM rs9806699 G>A had a protective effect against SIM (OR = 0.80, 95% CI 0.68–0.94, P = 0.006, I2 = 17.5%). There was no statistically heterogeneity according to the Q test (P = 0.301) and the I2 statistic (Fig. 2). The effect of GATM rs9806699 G>A was further evaluated in a subgroup analysis of severe SIM. When the three eligible studies with severe SIM subgroups were pooled, the GATM rs9806699 polymorphism was found to be not associated with a risk of severe SIM (OR = 0.84, 95% CI 0.65–1.09, P = 0.187, I2 = 0%) (Fig. 3). Then, in order to exclude the influence of fibrates or niacin, we assessed the effect of GATM rs9806699 G>A in subgroups with fibrates or niacin comedications excluded or not (Fig. 4). The results reached statistically significant in the subgroup with fibrates or niacin comedications excluded (OR = 0.76, 95% CI 0.60–0.96, P = 0.023, I2 = 0%), but not significant in the subgroup that not excluding fibrates or niacin uses (OR = 0.84, 95% CI 0.67–1.04, P = 0.102, I2 = 55.3%).

Forest plot of pooled fix-effects-based OR with 95% CI from six studies of association between GATM rs9806699 G>A and SIM, comparing SIM case versus control. *MAF at rs9806699 refers to allele frequency for A allele. CI, confidence interval; OR, odds ratio; SIM, statin-induced myopathy; GATM, glycine amidinotransferase gene; MAF, minor allele frequency

Forest plot of pooled fix-effects-based OR with 95% CI from three studies of association between GATM rs9806699 G>A and severe SIM, assessing severe SIM subgroup versus control. *MAF at rs9806699 refers to allele frequency for A allele. **This value was calculated by odds ratio (OR) of MAF between cases and control (OR = 0.94). CI, confidence interval; OR, odds ratio; SIM, statin-induced myopathy; GATM, glycine amidinotransferase gene; MAF, minor allele frequency

Forest plot of pooled fix-effects-based OR with 95% CI from six studies of association between GATM rs9806699 G>A and SIM in subgroup with fibrates or niacin comedications excluded or not, assessing case versus control. *MAF at rs9806699 refers to allele frequency for A allele. CI, confidence interval; OR, odds ratio; SIM, statin-induced myopathy; GATM, glycine amidinotransferase gene; MAF, minor allele frequency
The effect of GATM rs9806699 G>A was also analyzed in different populations (eFig. 1). The result was statistically significant in the western subgroup (OR = 0.82, 95% CI 0.68–0.98, P = 0.030, I2 = 0%), but not significant in the Asian subgroup (OR = 0.74, 95% CI 0.53–1.04, P = 0.081, I2 = 72.7%). GATM rs9806699 G>A was found to be associated with decreased risk of SIM only in studies using elevation of CK levels as a necessary condition for diagnosis criteria of SIM (OR = 0.81, 95% CI 0.66–0.99, P = 0.042, I2 = 4.3%) (eFig. 2).
The association between GATM rs1719247 and rs1346268 with statin-induced myopathy
We further examined variation at the association of other two SNPs, rs1719247 and rs1346268, with risk of SIM. Three studies investigating the association between GATM rs1719247 C>T and SIM was included and combined in a fixed-effects meta-analysis (Fig. 5a). The results indicated that variation at rs1719247 C>T was associated with the risk of SIM (OR = 0.69, 95% CI 0.55–0.87, P = 0.002, I2 = 39.6%). Similarly, the association of rs1346268 T>C with SIM was also significant (OR = 0.69, 95% CI 0.55–0.87, P = 0.002, I2 = 0%) (Fig. 5b). There was no statistical heterogeneity at rs1719247 and rs1346268 (Fig. 5).

Forest plot of pooled fix-effects-based OR with 95% CI from three studies of association between GATM rs1719247 (a), GATM rs1346268 (b), and SIM, comparing SIM case versus control. *MAF at rs1719247 and rs1346268 refers to allele frequency for T and C allele, respectively. CI, confidence interval; OR, odds ratio; SIM, statin-induced myopathy; GATM, glycine amidinotransferase gene; MAF, minor allele frequency
Sensitivity analysis
Among the six included studies, Floyd’s study evaluated only cerivastatin, which was voluntarily withdrawn due to a high rate of drug-related rhabdomyolysis and no longer available in the clinical practice, while Bai’s study focused on rosuvastatin, which is a hydrophilic type of statins that has been reported to have fewer SIM adverse events than lipophilic statins. Sensitivity analysis was conducted by excluding these two studies, respectively. The effect of GATM rs9806699 remained significant after excluding Floyd’s study (OR = 0.80, 95% CI 0.67–0.95, P = 0.013) (eFig. 3), and it was marginally significant after excluding Bai’s study (OR = 0.84, 95% CI 0.71–1.00, P = 0.051) (eFig. 4).
Publication bias
-
Publication bias, evaluated by funnel plot, was shown in Fig. 6. All studies were in the 95% confidence limits and the plot showed good symmetry. Therefore, no significant publication bias was detected.

Funnel plots of the meta-analysis of the relationship between GATM rs9806699 G>A and SIM. CI, confidence interval; OR, odds ratio; SIM, statin-induced myopathy; GATM, glycine amidinotransferase gene
Discussion
Our meta-analysis showed that GATM rs9806699 G>A was associated with decreased risk of SIM. This association remained significant in the subgroup with fibrates or niacin excluded, indicating that GATM rs9806699 G>A might be an independent protective factor for SIM. The association of rs9806699 G>A with severe SIM was not significant. Furthermore, other two SNPs of GATM, rs1719247 C>T and rs1346268 T>C were also related to reduced risk of SIM. Our meta-analysis addresses the previous controversy and clarified the effect of GATM polymorphism on SIM, which may help to better understand the underlying mechanism of SIM and contribute to individual risk stratification for statin users.
A protective effect of GATM rs9806699 G>A was observed in our present meta-analysis. This correlation was firstly reported by Mangravite et al. in 2013. By using gene expression profiling of lymphoblastoid cell lines derived from 480 participants treated with simvastatin, they identified that an eQTL for GATM, rs9806699, interacted with simvastatin exposure. GATM rs9806699 G>A was further found to be associated with decreased incidence of SIM in their study population of 72 cases and 220 controls, which were matched based on statin exposure, age, and gender [10]. However, subsequent studies yielded conflict results [11,12,13,14,15]. Luzum et al. [13] and Sai et al. [14] only used “muscle symptoms” as diagnosis of cases in their study without considering CK levels. Our subgroup analysis indicated that the effects of GATM rs9806699 were only significant in studies using CK levels as criteria. Cases in Floyd et al.’s [12] study were all severe cases with CK levels> 10 × ULN and muscle symptoms, while SIM cases of Mangravite et al. were incipient. It was possible that this GATM variant only protect against mild but not severe SIM. Other differences in the study populations might also lead to inconsistent results.
The association of variations at another two SNPs, rs1719247 and rs1346268, with SIM has also been investigated. In the Study of Effectiveness of Additional Reductions in Cholesterol and Homocysteine (SEARCH) with 100 myopathy cases, both of variations at rs1719247 and rs1346268 was associated with decreased risk of SIM [10]. Mangravite et al. also verified the protective effect of variation at rs1719247 in another independent population with 72 cases [10]. However, Floyd et al. could not replicate these results in their case-control study [12]. As a result, we included these three studies and verified that of both rs1719247 C>T and rs1346268 T>C were also protective factors for SIM. These two SNPs are in linkage disequilibrium with rs9806699 [10], so the association between these two SNPs and SIM might be similar to that of rs9806699 [21]. But, how variations at these two SNPs affect the expression of GATM and thereby influence the occurrence of SIM is still unclear.
To investigate potential factors modifying the effect of GATM polymorphism, we performed subgroup analyses of severe SIM cases, with data from studies of Car et al. [11], Floyd et al. [12], and severe subgroup of Luzum.et al. [13] combined together. No association was found between GATM rs9806699 polymorphism and risk of severe SIM with no heterogeneity within included studies. These results indicated that GATM rs9806699 G>A might only exert protect effect against mild but not severe SIM. Regarding that all cases in the study of Mangravite et al. [10] were incipient myopathy, it might be explained why their results could not be replicated in case-control studies of severe cases or our subgroup analysis. However, there has been few separate studies for mild cases, and some studies have not distinguished between severe and mild cases, it is difficult for us to perform a subgroup analysis for mild cases with enough studies included. Furthermore, the definition of severe cases was not uniform, which might affect the effect of GATM rs9806699 variation. Therefore, a larger study with an accurate definition of the severity of myopathy is required. Because fibrates and niacin were considered to increase incidence of SIM and they were commonly used as comedication of statin in patients with dyslipidemia [10, 22,23,24], we evaluated the effect of rs9806699 in subgroups excluding fibrates or niacin. We found that the protective effect of rs9806699 G>A was significant without usage of fibrates or niacin. Due to the promoting effect on SIM of fibrates and niacin, they would mask the protective effect of G>A at GATM rs9806699. That provided an explanation for our negative pooled results in subgroup that not excluding fibrates or niacin. So, this finding alerted researchers the necessity of excluding the effects of drugs like fibrates or niacin as much as possible in the future. There was a significant association between GATM rs9806699 G>A and SIM in western subgroup but not in Asian subgroup. The insufficient studies at present among Asian population might lead to the non-significant result, thus more evidence in Asian population is needed.
Our meta-analysis has some limitations. First, owing to a lack of standard definition of SIM, there is heterogeneity in the diagnosis of SIM in included studies. Larger sample studies with widely accepted definition of SIM are needed to further verify the effect of GATM polymorphism. Second, due to the limited studies regarding the association of GATM polymorphism and SIM to date, subgroup analysis for potential influencing factors like statin types,or statin doses cannot be performed. Different races with genetic diversity may also be an influencing factor, unfortunately it is not feasible to draw a conclusion because there is not enough data available for subgroup analysis. Lack of original data of individual patient in our meta-analysis restricted further subgroup analyses and interpretation of differences between studies. However, our study is the largest sample size of meta-analysis to investigate the association between GATM polymorphisms and SIM, and also the first one to perform subgroup analysis according to the severity of myopathy and comedications. Larger sample studies with standardized genotyping methods at different SNP sites of GATM and accurate definition of SIM severity are warranted to further verify its protective effect on SIM. Third, all of the included studies are case-control studies because there is lack of prospective study to date. Therefore, a well-designed prospective study should be performed in the future, with other co-variants like demographic characteristics, statin dose, types, and period of treatment considered.
Conclusion
In conclusion, our meta-analysis has indicated that GATM polymorphism is associated with the risk of SIM. Variations including rs9806699 G>A, rs1719247 C>T. and rs1346268 T>C may be protective factors of SIM. Subgroup analysis has shown that fibrates or niacin may mask its protective effect and should be excluded in future studies. The association of rs9806699 G>A with severe SIM become non-significant in subgroup analysis, indicating that it may only exert protective effect on mild SIM cases. Our study provides new insight into the genetic determinants of SIM and identification of at-risk population, which may help to reduce the incidence of SIM and optimize statin adherence.
References
Cohen JD, Brinton EA, Ito MK, Jacobson TA (2012) Understanding statin use in America and gaps in patient education (USAGE): an internet-based survey of 10,138 current and former statin users. J Clin Lipidol 6(3):208–215. https://doi.org/10.1016/j.jacl.2012.03.003
Ekhart C, de Jong L, Gross-Martirosyan L, van Hunsel F (2016) Muscle rupture associated with statin use. Br J Clin Pharmacol 82(2):473–477. https://doi.org/10.1111/bcp.12973
Newman CB, Preiss D, Tobert JA, Jacobson TA, Page RL 2nd, Goldstein LB, Chin C, Tannock LR, Miller M, Raghuveer G, Duell PB, Brinton EA, Pollak A, Braun LT, Welty FK, American Heart Association Clinical Lipidology LM, Thrombosis Committee aJCotCoAT, Vascular B, Council on L, Cardiometabolic H, Council on Cardiovascular Disease in the Y, Council on Clinical C, Stroke C (2019) Statin safety and associated adverse events: a scientific statement from the American Heart Association. Arterioscler Thromb Vasc Biol 39(2):e38–e81. https://doi.org/10.1161/ATV.0000000000000073
Adhyaru BB, Jacobson TA (2018) Safety and efficacy of statin therapy. Nat Rev Cardiol 15(12):757–769. https://doi.org/10.1038/s41569-018-0098-5
El-Salem K, Ababneh B, Rudnicki S, Malkawi A, Alrefai A, Khader Y, Saadeh R, Saydam M (2011) Prevalence and risk factors of muscle complications secondary to statins. Muscle Nerve 44(6):877–881. https://doi.org/10.1002/mus.22205
Brunham LR, Baker S, Mammen A, Mancini GBJ, Rosenson RS (2018) Role of genetics in the prediction of statin-associated muscle symptoms and optimization of statin use and adherence. Cardiovasc Res 114(8):1073–1081. https://doi.org/10.1093/cvr/cvy119
Link E, Parish S, Armitage J, Bowman L, Heath S, Matsuda F, Gut I, Lathrop M, Collins R (2008) SLCO1B1 variants and statin-induced myopathy--a genomewide study. N Engl J Med 359(8):789–799. https://doi.org/10.1056/NEJMoa0801936
Khan A, Tian L, Zhang C, Yuan K, Xu S (2016) Genetic diversity and natural selection footprints of the glycine amidinotransferase gene in various human populations. Sci Rep 6:18755. https://doi.org/10.1038/srep18755
Ballard KD, Thompson PD (2013) Does reduced creatine synthesis protect against statin myopathy? Cell Metab 18(6):773–774. https://doi.org/10.1016/j.cmet.2013.11.012
Mangravite LM, Engelhardt BE, Medina MW, Smith JD, Brown CD, Chasman DI, Mecham BH, Howie B, Shim H, Naidoo D, Feng Q, Rieder MJ, Chen YD, Rotter JI, Ridker PM, Hopewell JC, Parish S, Armitage J, Collins R, Wilke RA, Nickerson DA, Stephens M, Krauss RM (2013) A statin-dependent QTL for GATM expression is associated with statin-induced myopathy. Nature 502(7471):377–380. https://doi.org/10.1038/nature12508
Carr DF, Alfirevic A, Johnson R, Chinoy H, van Staa T, Pirmohamed M (2014) GATM gene variants and statin myopathy risk. Nature 513(7518):E1. https://doi.org/10.1038/nature13628
Floyd JS, Bis JC, Brody JA, Heckbert SR, Rice K, Psaty BM (2014) GATM locus does not replicate in rhabdomyolysis study. Nature 513(7518):E1–E3. https://doi.org/10.1038/nature13629
Luzum JA, Kitzmiller JP, Isackson PJ, Ma C, Medina MW, Dauki AM, Mikulik EB, Ochs-Balcom HM, Vladutiu GD (2015) GATM polymorphism associated with the risk for statin-induced myopathy does not replicate in case-control analysis of 715 dyslipidemic individuals. Cell Metab 21(4):622–627. https://doi.org/10.1016/j.cmet.2015.03.003
Sai K, Kajinami K, Akao H, Iwadare M, Sato-Ishida R, Kawai Y, Takeda K, Tanimoto T, Yamano T, Akasaka T, Ishida T, Hirata KI, Saku K, Yagi S, Soeki T, Sata M, Ueno M, Miyazaki S, Shiraki A, Oyama JI, Node K, Sugamura K, Ogawa H, Kurose K, Maekawa K, Matsuzawa Y, Imatoh T, Hasegawa R, Saito Y (2016) A possible role for HLA-DRB1*04:06 in statin-related myopathy in Japanese patients. Drug Metab Pharmacokinet 31(6):467–470. https://doi.org/10.1016/j.dmpk.2016.09.002
Bai X, Zhang B, Wang P, Wang GL, Li JL, Wen DS, Long XZ, Sun HS, Liu YB, Huang M, Zhong SL (2019) Effects of SLCO1B1 and GATM gene variants on rosuvastatin-induced myopathy are unrelated to high plasma exposure of rosuvastatin and its metabolites. Acta Pharmacol Sin 40(4):492–499. https://doi.org/10.1038/s41401-018-0013-y
Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. Jama 283(15):2008–2012. https://doi.org/10.1001/jama.283.15.2008
Wells GA SB, O’Connell (2011) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analysis. The Ottawa Hospital Research Institute. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
Lau J, Ioannidis JP, Schmid CH (1997) Quantitative synthesis in systematic reviews. Ann Intern Med 127(9):820–826. https://doi.org/10.7326/0003-4819-127-9-199711010-00008
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327(7414):557–560. https://doi.org/10.1136/bmj.327.7414.557
Sutton AJ, Duval SJ, Tweedie RL, Abrams KR, Jones DR (2000) Empirical assessment of effect of publication bias on meta-analyses. BMJ 320(7249):1574–1577. https://doi.org/10.1136/bmj.320.7249.1574
Carlton VE, Ireland JS, Useche F, Faham M (2006) Functional single nucleotide polymorphism-based association studies. Hum Genomics 2(6):391–402. https://doi.org/10.1186/1479-7364-2-6-391
Camerino GM, Pellegrino MA, Brocca L, Digennaro C, Camerino DC, Pierno S, Bottinelli R (2011) Statin or fibrate chronic treatment modifies the proteomic profile of rat skeletal muscle. Biochem Pharmacol 81(8):1054–1064. https://doi.org/10.1016/j.bcp.2011.01.022
Graham DJ, Staffa JA, Shatin D, Andrade SE, Schech SD, La Grenade L, Gurwitz JH, Chan KA, Goodman MJ, Platt R (2004) Incidence of hospitalized rhabdomyolysis in patients treated with lipid-lowering drugs. Jama 292(21):2585–2590. https://doi.org/10.1001/jama.292.21.2585
Saxon DR, Eckel RH (2016) Statin intolerance: a literature review and management strategies. Prog Cardiovasc Dis 59(2):153–164. https://doi.org/10.1016/j.pcad.2016.07.009
Funding
This study was supported by the Key Laboratory of Molecular Cardiovascular Sciences (Peking University), Ministry of Education.
Author information
Authors and Affiliations
Contributions
Mengyuan Liu and Jianping Li conceived and designed the study; Mengyuan Liu and Fangfang Fan accomplished the literature search and selection. Mengyuan Liu and Yan Zhang performed the data extraction and analysis. Mengyuan Liu drafted the manuscript and all authors critically revised it. Jianping Li supervised the whole study. The submitted manuscript was read and approved by all of the authors.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval and consent to participate
No ethics approval or consent to participate was required as this is a meta-analysis.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, M., Fan, F., Zhang, Y. et al. The association of GATM polymorphism with statin-induced myopathy: a systematic review and meta-analysis. Eur J Clin Pharmacol 77, 349–357 (2021). https://doi.org/10.1007/s00228-020-03019-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-020-03019-3