
Abstract
Background and objectives
Dosing of vancomycin in pediatric patients undergoing continuous venous–venous hemodiafiltration (CVVHDF) is challenging. Characterization of vancomycin pharmacokinetics can assist with dosing and attainment of goal serum concentrations.
Design, setting, participants, and measurements
Patients less than 19 years of age who received vancomycin and had post-dose vancomycin concentrations while undergoing CVVHDF were identified. Data collection included the following: patient demographics, vancomycin dosing and serum concentrations, CVVHDF variables, serum creatinine (SCR), blood urea nitrogen (BUN), albumin, hematocrit, and urine output. Fat-free mass was calculated. Data were summarized with descriptive statistical methods, and population pharmacokinetic analysis was performed with NONMEM 7.2 and PDx-Pop 5.2. Simulation was performed to identify dosing regimens with the highest percentage of goal serum concentration < 20 mg/L and AUC0–24:MIC ≥ 400 attainment.
Results
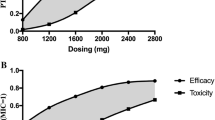
A total of 138 patients met study criteria (45.6% male, median age 4.9 years (IQR (1.0, 14.5))). Mean vancomycin dose was 14.3 ± 1.6 mg/kg/dose (19.5 ± 3.0 mg/kg/dose by FFM). Patients had a median of six (IQR 2, 12) vancomycin serum concentrations sampled 13.6 ± 8.4 h after the dose, and the mean vancomycin serum concentration was 11.3 ± 3.4 mg/L. Vancomycin pharmacokinetics were characterized by a two-compartment model with allometric scaling on fat-free mass and significant covariates of SCR, BUN, dialysate flow rate, and ultrafiltration rate on clearance. Simulation identified doses of 40–50 mg/kg/day that divided every 8–12 h had the highest percentage of patients with a serum concentration < 20 mg/L and an AUC0–24:MIC ≥ 400.
Conclusions
Vancomycin pharmacokinetics are characterized by fat-free mass, serum creatinine, blood urea nitrogen, dialysate flow rate, and ultrafiltration rate in the pediatric CVVHDF population. Dosing of 40–50 mg/kg/day on fat-free mass divided every 8–12 h with frequent vancomycin serum sampling is recommended.


Similar content being viewed by others

References
Wilson FP, Berns JS (2012) Vancomycin levels are frequently subtherapeutic during continuous venovenous hemodialysis (CVVHD). Clin Nephrol 77:329–331
Omrani AS, Mously A, Cabaluna MP, Kawas J, Albarrak MM, Alfahad WA (2015) Vancomycin therapy in critically ill patients on continuous renal replacement therapy; are we doing enough? Saudi Pharm J 23:327–329
Jamal JA, Udy AA, Lipman J, Roberts JA (2014) The impact of variation in renal replacement therapy settings on piperacillin, meropenem, and vancomycin drug clearance in the critically ill: an analysis of published literature and dosing regimens. Crit Care Med 42:1640–1650
Joy MS, Matzke GR, Frye RF, Palevsky PM (1998) Determinants of vancomycin clearance by continuous venovenous hemofiltration and continuous venovenous hemodialysis. Am J Kidney Dis 31:1019–1027
Roberts DM, Roberts JA, Roberts MS, Liu X, Nair P, Cole L, Lipman J, Bellomo R, RENAL Replacement Therapy Study Investigators (2012) Variability of antibiotic concentrations in critically ill patients receiving continuous renal replacement therapy: a multicentre pharmacokinetic study. Crit Care Med 40:1523–1528
Trotman RL, Williamson JC, Shoemaker DM, Salzer WL (2005) Antibiotic dosing in critically ill adult patients receiving continuous renal replacement therapy. Clin Infect Dis 41:1159–1166
Uchino S, Cole L, Morimatsu H, Goldsmith D, Bellomo R (2002) Clearance of vancomycin during high-volume haemofiltration: impact of pre-dilution. Intensive Care Med 28:1664–1667
Boereboom FT, Ververs FF, Blankestijn PJ, Savelkoul TJ, van Dijk A (1999) Vancomycin clearance during continuous venovenous haemofiltration in critically ill patients. Intensive Care Med 25:1100–1104
Chaijamorn W, Jitsurong A, Wiwattanawongsa K, Wanakamanee U, Dandecha P (2011) Vancomycin clearance during continuous venovenous haemofiltration in critically ill patients. Int J Antimicrob Agents 38:152–156
Petejova N, Martinek A, Zahalkova J, Duricova J, Brozmannova H, Urbanek K, Grundmann M, Plasek J, Kacirova I (2014) Vancomycin pharmacokinetics during high-volume continuous venovenous hemofiltration in critically ill septic patients. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 158:65–72
Cies JJ, Moore WS 2nd, Conley SB et al (2016) Continuous infusion vancomycin through the addition of vancomycin to the continuous renal replacement therapy solution in the PICU: a case series. Pediatr Crit Care Med 17:e138–e145
Anderson BJ, Holford NH (2008) Mechanism-based concepts of size and maturity in pharmacokinetics. Annu Rev Pharmacol Toxicol 48:303–332
Anderson BJ, Holford NH (2009) Mechanistic basis of using body size and maturation to predict clearance in humans. Drug Metab Pharmacokinet 24:25–36
Anderson BJ, Holford NH (2013) Understanding dosing: children are small adults, neonates are immature children. Arch Dis Child 98:737–744
Rybak M, Lomaestro B, Rotschafer JC, Moellering R Jr, Craig W, Billeter M, Dalovisio JR, Levine DP (2009) Therapeutic monitoring of vancomycin in adult patients: a consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am J Health Syst Pharm 66:82–98
Al-Sallami HS, Goulding A, Grant A, Taylor R, Holford N, Duffull SB (2015) Prediction of fat-free mass in children. Clin Pharmacokinet 54:1169–1178
Ogden CL, Carroll MD, Lawman HG, Fryar CD, Kruszon-Moran D, Kit BK, Flegal KM (2016) Trends in obesity prevalence among children and adolescents in the United States, 1988-1994 through 2013-2014. Jama 315:2292–2299
Beumier M, Roberts JA, Kabtouri H, Hites M, Cotton F, Wolff F, Lipman J, Jacobs F, Vincent JL, Taccone FS (2013) A new regimen for continuous infusion of vancomycin during continuous renal replacement therapy. J Antimicrob Chemother 68:2859–2865
DelDot ME, Lipman J, Tett SE (2004) Vancomycin pharmacokinetics in critically ill patients receiving continuous venovenous haemodiafiltration. Br J Clin Pharmacol 58:259–268
Escobar L, Andresen M, Downey P, Gai MN, Regueira T, Bórquez T, Lipman J, Roberts JA (2014) Population pharmacokinetics and dose simulation of vancomycin in critically ill patients during high-volume haemofiltration. Int J Antimicrob Agents 44:163–167
Beal SL (2002) Commentary on significance levels for covariate effects in NONMEM. J Pharmacokinet Pharmacodyn 29:403–410 discussion 11-2
Hooker AC, Staatz CE, Karlsson MO (2007) Conditional weighted residuals (CWRES): a model diagnostic for the FOCE method. Pharm Res 24:2187–2197
Karlsson MO, Savic RM (2007) Diagnosing model diagnostics. Clin Pharmacol Ther 82:17–20
Le J, Bradley JS, Murray W et al (2013) Improved vancomycin dosing in children using area under the curve exposure. Pediatr Infect Dis J 32:e155–e163
Udy AA, Covajes C, Taccone FS, Jacobs F, Vincent JL, Lipman J, Roberts JA (2013) Can population pharmacokinetic modelling guide vancomycin dosing during continuous renal replacement therapy in critically ill patients? Int J Antimicrob Agents 41:564–568
Roberts DM, Liu X, Roberts JA et al (2015) A multicenter study on the effect of continuous hemodiafiltration intensity on antibiotic pharmacokinetics. Crit Care (London, England) 19:84
Marsot A, Boulamery A, Bruguerolle B, Simon N (2012) Vancomycin: a review of population pharmacokinetic analyses. Clin Pharmacokinet 51:1–13
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Institutional review board approval from Baylor College of Medicine and affiliated institutions was obtained
Conflict of interest
The authors are currently receiving NIH funding for a prospective population pharmacokinetic trial of vancomycin in pediatrics.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix 1 Fat-free mass calculation
Appendix 1 Fat-free mass calculation
- WT:
-
weight (kg)
- Age:
-
age in years
- BMI:
-
body mass index (kg/m2)
Rights and permissions
About this article

Cite this article
Moffett, B.S., Morris, J., Munoz, F. et al. Population pharmacokinetic analysis of vancomycin in pediatric continuous renal replacement therapy. Eur J Clin Pharmacol 75, 1089–1097 (2019). https://doi.org/10.1007/s00228-019-02664-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-019-02664-7