
Abstract
Purpose
The aim of this study was to describe persistence with vitamin K antagonist (VKA) treatment in German atrial fibrillation (AF) patients and to identify factors which may be associated with early discontinuation of VKA therapy.
Methods
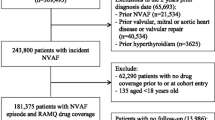
We did a retrospective cohort study based on an anonymized German claims dataset with VKA treatment-naïve AF patients, who received at least one VKA prescription. VKA therapy discontinuation was defined as a gap >180 days.
Results
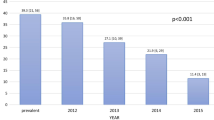
We identified 38,076 VKA patients who started a VKA therapy (mean age 76.13 years; 56.08% female; mean CHA2DS2-VASc-Score 4.49; mean Charlson Comorbidity Index (CCI) 3.91). After four quarters since start of VKA treatment, 14,889 (39.10%) of observed patients had discontinued their VKA treatment (after eight quarters: 54.61%). Mean time until treatment discontinuation was 390.55 days. Risk of VKA discontinuation increased with the diagnosis of dementia within the first two quarters of VKA treatment [HR 1.35 (95% CI 1.29–1.40)], diagnosed alcohol or drug abuse in the baseline period [HR 1.25; 95% CI 1.18–1.33)], female gender [HR 1.08; 95% CI 1.05–1.10)], higher age (HR 1.03; 95% CI 1.03–1.03), higher CCI (HR 1.05; 95% CI 1.04–1.05), any prescription of NSAID (HR 1.07; 95% CI 1.04–1.10), and number of surgeries in the first two quarters of VKA treatment (HR 1.05; 95% CI 1.04–1.05). At least one yearly visit to a cardiologist since start of VKA treatment decreased the risk of non-persistence [HR 0.90; 95% CI 0.88–0.93] and a cancer diagnosis in the baseline period (HR 0.92; 95% CI 0.89–0.96).
Conclusion
Non-persistence related to VKA therapy is common in AF patients. Older more comorbid female patients as well as patients who face surgeries and who do not visit a cardiologist regularly face a higher therapy discontinuation risk.

Similar content being viewed by others

References
Heeringa J, van der Kuip DAM, Hofman A et al (2006) Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur Heart J 27(8):949–953. doi:10.1093/eurheartj/ehi825
Schnabel RB, Sullivan LM, Levy D et al (2009) Development of a risk score for atrial fibrillation (Framingham Heart Study): a community-based cohort study. Lancet 373(9665):739–745. doi:10.1016/S0140-6736(09)60443-8
Fang MC, Go AS, Chang Y et al (2008) Comparison of risk stratification schemes to predict thromboembolism in people with nonvalvular atrial fibrillation. J Am Coll Cardiol 51(8):810–815. doi:10.1016/j.jacc.2007.09.065
Lip GYH, Laroche C, Ioachim PM et al (2014) Prognosis and treatment of atrial fibrillation patients by European cardiologists: one year follow-up of the EURObservational Research Programme-Atrial Fibrillation General Registry Pilot Phase (EORP-AF Pilot registry). Eur Heart J 35(47):3365–3376. doi:10.1093/eurheartj/ehu374
Fuster V, Ryden LE, Cannom DS et al (2011) 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 123(10):e269–e367. doi:10.1161/CIR.0b013e318214876d
Lip GYH, Rudolf M, Kakar P (2007) Management of atrial fibrillation: the NICE guidelines. Int J Clin Pract 61(1):9–11. doi:10.1111/j.1742-1241.2006.01151.x
You JJ, Singer DE, Howard PA et al (2012) Antithrombotic therapy for atrial fibrillation: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 141(2 Suppl):75. doi:10.1378/chest.11-2304
Kirchhof P, Benussi S, Kotecha D et al (2016) 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 37(38):2893–2962. doi:10.1093/eurheartj/ehw210
Nieuwlaat R, Capucci A, Lip GYH et al (2006) Antithrombotic treatment in real-life atrial fibrillation patients: a report from the Euro Heart Survey on Atrial Fibrillation. Eur Heart J 27(24):3018–3026. doi:10.1093/eurheartj/ehl015
Mohammed MA, Marshall T, Nirantharakumar K et al (2013) Patterns of warfarin use in subgroups of patients with atrial fibrillation: a cross-sectional analysis of 430 general practices in the United Kingdom. PLoS One 8(5):e61979. doi:10.1371/journal.pone.0061979
Kirchhof P, Ammentorp B, Darius H et al (2014) Management of atrial fibrillation in seven European countries after the publication of the 2010 ESC guidelines on atrial fibrillation: primary results of the PREvention oF thromboemolic events--European Registry in Atrial Fibrillation (PREFER in AF). Europace 16(1):6–14. doi:10.1093/europace/eut263
Deitelzweig SB, Buysman E, Pinsky B et al (2013) Warfarin use and stroke risk among patients with nonvalvular atrial fibrillation in a large managed care population. Clin Ther 35(8):1201–1210. doi:10.1016/j.clinthera.2013.06.005
Wilke T, Groth A, Mueller S et al (2012) Oral anticoagulation use by patients with atrial fibrillation in Germany. Adherence to guidelines, causes of anticoagulation under-use and its clinical outcomes, based on claims-data of 183,448 patients. Thromb Haemost 107(6):1053–1065. doi:10.1160/TH11-11-0768
Wilke T, Groth A, Pfannkuche M et al (2015) Real life anticoagulation treatment of patients with atrial fibrillation in Germany: extent and causes of anticoagulant under-use. J Thromb Thrombolysis 40(1):97–107. doi:10.1007/s11239-014-1136-8
Zalesak M, Siu K, Francis K et al (2013) Higher persistence in newly diagnosed nonvalvular atrial fibrillation patients treated with dabigatran versus warfarin. Circ Cardiovasc Qual Outcomes 6(5):567–574. doi:10.1161/CIRCOUTCOMES.113.000192
Suh D-C, Choi JC, Schein J et al (2013) Factors associated with warfarin discontinuation, including bleeding patterns, in atrial fibrillation patients. Curr Med Res Opin 29(7):761–771. doi:10.1185/03007995.2013.795142
Song X, Sander SD, Varker H et al (2012) Patterns and predictors of use of warfarin and other common long-term medications in patients with atrial fibrillation. Am J Cardiovasc Drugs 12(4):245–253. doi:10.2165/11632540-000000000-00000
Hansen CM, Olesen JB, Hansen ML et al (2012) Initiation and persistence with warfarin therapy in atrial fibrillation according to ethnicity. Front Pharmacol 3:123. doi:10.3389/fphar.2012.00123
Gallagher AM, Rietbrock S, Plumb J et al (2008) Initiation and persistence of warfarin or aspirin in patients with chronic atrial fibrillation in general practice: do the appropriate patients receive stroke prophylaxis? J Thromb Haemost 6(9):1500–1506. doi:10.1111/j.1538-7836.2008.03059.x
Lip GYH (2011) Implications of the CHA(2)DS(2)-VASc and HAS-BLED scores for thromboprophylaxis in atrial fibrillation. Am J Med 124(2):111–114. doi:10.1016/j.amjmed.2010.05.007
WHO Collaborating Centre for Drug Statistics Methodology (2010) Guidelines for ATC classification and DDD assignment: 2011. Norwegian Institute of Public Health, Oslo
Forslund T, Wettermark B, Hjemdahl P (2016) Comparison of treatment persistence with different oral anticoagulants in patients with atrial fibrillation. Eur J Clin Pharmacol 72(3):329–338. doi:10.1007/s00228-015-1983-z
Fang MC, Go AS, Chang Y et al (2010) Warfarin discontinuation after starting warfarin for atrial fibrillation. Circ Cardiovasc Qual Outcomes 3(6):624–631. doi:10.1161/CIRCOUTCOMES.110.937680
Chae J-W, Song CS, Kim H et al (2011) Prediction of mortality in patients undergoing maintenance hemodialysis by Charlson Comorbidity Index using ICD-10 database. Nephron Clin Pract 117(4):c379–c384. doi:10.1159/000321525
Sorensen SV, Dewilde S, Singer DE et al (2009) Cost-effectiveness of warfarin: trial versus “real-world” stroke prevention in atrial fibrillation. Am Heart J 157(6):1064–1073. doi:10.1016/j.ahj.2009.03.022
Simpson SH, Eurich DT, Majumdar SR et al (2006) A meta-analysis of the association between adherence to drug therapy and mortality. BMJ 333(7557):15. doi:10.1136/bmj.38875.675486.55
Martinez C, Katholing A, Wallenhorst C et al (2016) Therapy persistence in newly diagnosed non-valvular atrial fibrillation treated with warfarin or NOAC. A cohort study. Thromb Haemost 115(1):31–39. doi:10.1160/TH15-04-0350
Casciano JP, Dotiwala ZJ, Martin BC et al (2013) The costs of warfarin underuse and nonadherence in patients with atrial fibrillation: a commercial insurer perspective. J Manag Care Pharm 19(4):302–316. doi:10.18553/jmcp.2013.19.4.302
Beyer-Westendorf J, Ehlken B, Evers T (2016) Real-world persistence and adherence to oral anticoagulation for stroke risk reduction in patients with atrial fibrillation. Europace. doi:10.1093/europace/euv421
Bjorck F, Renlund H, Svensson PJ et al (2015) Warfarin persistence among stroke patients with atrial fibrillation. Thromb Res 136(4):744–748. doi:10.1016/j.thromres.2015.07.028
Koscielny J, Ziemer S, von Heymann C (2009) Patients with oral anticoagulation—bridging anticoagulation in the perioperative phase (Patienten unter oraler Antikoagulation—perioperatives bridging). Hamostaseologie 29(3):247–255
Siegal D, Yudin J, Kaatz S et al (2012) Periprocedural heparin bridging in patients receiving vitamin K antagonists: systematic review and meta-analysis of bleeding and thromboembolic rates. Circulation 126(13):1630–1639. doi:10.1161/CIRCULATIONAHA.112.105221
Hylek EM, Evans-Molina C, Shea C et al (2007) Major hemorrhage and tolerability of warfarin in the first year of therapy among elderly patients with atrial fibrillation. Circulation 115(21):2689–2696. doi:10.1161/CIRCULATIONAHA.106.653048
Man-Son-Hing M, Laupacis A (2003) Anticoagulant-related bleeding in older persons with atrial fibrillation: physicians’ fears often unfounded. Arch Intern Med 163(13):1580–1586. doi:10.1001/archinte.163.13.1580
Ezekowitz MD, Falk RH (2004) The increasing need for anticoagulant therapy to prevent stroke in patients with atrial fibrillation. Mayo Clin Proc 79(7):904–913. doi:10.1016/S0025-6196(11)62158-7
Wilke T, Bauer S, Mueller S et al (2016) Patient preferences for oral anticoagulation therapy in atrial Fibrillation: A Systematic Literature Review. Patient. doi:10.1007/s40271-016-0185-9
Bottger B, Thate-Waschke I-M, Bauersachs R et al (2015) Preferences for anticoagulation therapy in atrial fibrillation: the patients’ view. J Thromb Thrombolysis 40(4):406–415. doi:10.1007/s11239-015-1263-x
Lefevre C, Benhaddi H, Lacoin L et al (2015) Persistence to vitamin-K antagonists (Vka) and novel oral anticoagulants (Noacs) in non-valvular atrial fibrillation (Nvaf): an observational study using a comprehensive regional database in Catalonia, Spain. Value Health 18(7):A403. doi:10.1016/j.jval.2015.09.938
Acknowledgements
The authors would like to thank two anonymous reviewers for their valuable comments.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Contributions of authors statement
All authors made substantial contributions to all of the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) final approval of the version to be submitted. Specifically, the main tasks the authors were engaged in were as follows:
TW and AG: project lead, participated in writing all parts of the paper, and statistical analysis.
UM and AF: conception/design of the study, data collection, validation of database, and interpretation of results in discussion section.
MP: conception/design of the study and interpretation of results in discussion section.
Funding
The study was funded by Boehringer Ingelheim Pharma GmbH, Germany. The study design, the collection/analysis of data, and the writing of the manuscript were done independently of the funding source.
Conflict of interest
Thomas Wilke has acted as consultant for Boehringer Ingelheim Pharma, Bayer, GSK, LEO Pharma, Novartis, Sanofi-Aventis, Bristol Myers Squibb, Pfizer, and other pharmaceutical companies. Antje Groth has no conflict of interest. Matthias Pfannkuche is employed by Boehringer Ingelheim Pharma (Germany). Ulf Maywald and Andreas Fuchs work for the insurance fund that provided the study data (AOK PLUS).
Electronic supplementary material
Supplemental Table A
(DOCX 51 kb).
Supplemental Table B
(DOCX 50 kb).
Rights and permissions
About this article

Cite this article
Wilke, T., Groth, A., Fuchs, A. et al. Persistence with VKA treatment in newly treated atrial fibrillation patients: an analysis based on a large sample of 38,076 German patients. Eur J Clin Pharmacol 73, 1437–1447 (2017). https://doi.org/10.1007/s00228-017-2307-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-017-2307-2