
Abstract
Summary
By investigating the relationship between serum testosterone, estradiol, and bone mineral density (BMD) in a large cohort of HIV-infected men, estradiol was associated with BMD, relative estrogen deficiency being involved in bone loss in men with hypogonadism, in addition to all HIV-related factors. Increased aromatization in adipose tissue does not counteract HIV-related bone loss.
Introduction
The purpose of this study is to evaluate the relationship between serum testosterone, estradiol, and BMD in a large cohort of HIV-infected men.
Methods
We investigated biochemical, hormonal parameters, and BMD in 1204 HIV-infected men (age 45.64 ± 7.33 years) participating in a cross-sectional, observational study. Among other parameters, the main outcome measures were serum total testosterone and estradiol, gonadotropins, 25-hydroxyvitamin D [25(OH)D], parathormone (PTH), calcium, phosphorous, femoral, and lumbar BMD.
Results
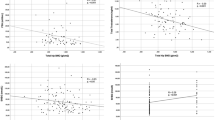
In men with HIV, the prevalence of osteoporosis and osteopenia is 15.1 and 63.2 % with 25(OH)D insufficiency being very common (60.1 %). After age adjustment, BMD is positively associated with estradiol, but not testosterone, at linear (p < 0.001) and stepwise (p < 0.05) multiple regression. Lumbar BMD significantly increases across the estradiol quartiles but not among testosterone quartiles. Femoral and lumbar BMD are significantly higher in men with estradiol ≥ 27 pg/mL than in those with estradiol <27 pg/mL. Apart from estradiol, only age, calcium, and BMI predict BMD at stepwise linear multiple regression, but the strength of this association is weak.
Conclusions
Estradiol, but not testosterone, is associated with BMD in HIV-infected men and exerts a protective role on bone especially when it is above 27 pg/mL. Relative estrogen deficiency is a potential mechanism involved in bone loss in hypogonadal HIV-infected men, in addition to all HIV-related factors. Increased aromatization in adipose tissue does not counteract HIV-related bone loss. Finally, reduced BMD in young-to-middle-aged HIV-infected men might be considered a peculiar hallmark of HIV infection due to its relevant prevalence, representing one of the several pieces composing the complicated puzzle of premature aging related to HIV infection.



Similar content being viewed by others


References
Brown TT, Qaqish RB (2006) Antiretroviral therapy and the prevalence of osteopenia and osteoporosis: a meta-analytic review. AIDS 20(17):2165–2174. doi:10.1097/QAD.0b013e32801022eb
Cotter AG, Powderly WG (2011) Endocrine complications of human immunodeficiency virus infection: hypogonadism, bone disease and tenofovir-related toxicity. Best Pract Res Clin Endocrinol Metab 25(3):501–515. doi:10.1016/j.beem.2010.11.003
Grijsen ML, Vrouenraets SM, Steingrover R, Lips P, Reiss P, Wit FW, Prins JM (2010) High prevalence of reduced bone mineral density in primary HIV-1-infected men. AIDS 24(14):2233–2238. doi:10.1097/QAD.0b013e32833c93fe
Rochira V, Zirilli L, Orlando G, Santi D, Brigante G, Diazzi C, Carli F, Carani C, Guaraldi G (2011) Premature decline of serum total testosterone in HIV-infected men in the HAART-era. PLoS One 6(12), e28512. doi:10.1371/journal.pone.0028512
Short CE, Shaw SG, Fisher MJ, Walker-Bone K, Gilleece YC (2014) Prevalence of and risk factors for osteoporosis and fracture among a male HIV-infected population in the UK. Int J STD AIDS 25(2):113–121. doi:10.1177/0956462413492714
Guerri-Fernandez R, Vestergaard P, Carbonell C, Knobel H, Aviles FF, Castro AS, Nogues X, Prieto-Alhambra D, Diez-Perez A (2013) HIV infection is strongly associated with hip fracture risk, independently of age, gender, and comorbidities: a population-based cohort study. J Bone Miner Res 28(6):1259–1263. doi:10.1002/jbmr.1874
Labarga P (2013) Bone mineral density loss, osteoporosis, and fractures in HIV. AIDS Rev 15(3):189–190
Ofotokun I, Weitzmann MN (2010) HIV-1 infection and antiretroviral therapies: risk factors for osteoporosis and bone fracture. Curr Opin Endocrinol Diabetes Obes 17(6):523–529. doi:10.1097/MED.0b013e32833f48d6
Brown TT (2013) HIV: an underrecognized secondary cause of osteoporosis? J Bone Miner Res 28(6):1256–1258. doi:10.1002/jbmr.1967
Rochira V, Guaraldi G (2014) Hypogonadism in the HIV-infected man. Endocrinol Metab Clin North Am 43(3):709–730. doi:10.1016/j.ecl.2014.06.005
Cazanave C, Dupon M, Lavignolle-Aurillac V, Barthe N, Lawson-Ayayi S, Mehsen N, Mercie P, Morlat P, Thiebaut R, Dabis F (2008) Reduced bone mineral density in HIV-infected patients: prevalence and associated factors. AIDS 22(3):395–402. doi:10.1097/QAD.0b013e3282f423dd
Rochira V, Balestrieri A, Madeo B, Zirilli L, Granata AR, Carani C (2006) Osteoporosis and male age-related hypogonadism: role of sex steroids on bone (patho)physiology. Eur J Endocrinol 154(2):175–185. doi:10.1530/eje.1.02088
Khosla S, Melton LJ 3rd, Riggs BL (2011) The unitary model for estrogen deficiency and the pathogenesis of osteoporosis: is a revision needed? J Bone Miner Res 26(3):441–451. doi:10.1002/jbmr.262
Rochira V, Kara E, Carani C (2015) The endocrine role of estrogens on human male skeleton. Int J Endocrinol 2015:165215. doi:10.1155/2015/165215
Rochira V, Carani C (2009) Aromatase deficiency in men: a clinical perspective. Nat Rev Endocrinol 5(10):559–568. doi:10.1038/nrendo.2009.176
Szulc P, Munoz F, Claustrat B, Garnero P, Marchand F, Duboeuf F, Delmas PD (2001) Bioavailable estradiol may be an important determinant of osteoporosis in men: the MINOS study. J Clin Endocrinol Metab 86(1):192–199. doi:10.1210/jcem.86.1.7126
Khosla S, Melton LJ 3rd, Robb RA, Camp JJ, Atkinson EJ, Oberg AL, Rouleau PA, Riggs BL (2005) Relationship of volumetric BMD and structural parameters at different skeletal sites to sex steroid levels in men. J Bone Miner Res 20(5):730–740. doi:10.1359/jbmr.041228
Mellstrom D, Vandenput L, Mallmin H, Holmberg AH, Lorentzon M, Oden A, Johansson H, Orwoll ES, Labrie F, Karlsson MK, Ljunggren O, Ohlsson C (2008) Older men with low serum estradiol and high serum SHBG have an increased risk of fractures. J Bone Miner Res 23(10):1552–1560. doi:10.1359/jbmr.080518
Khosla S (2008) Estrogen and bone: insights from estrogen-resistant, aromatase-deficient, and normal men. Bone 43(3):414–417. doi:10.1016/j.bone.2008.05.005
Lanfranco F, Zirilli L, Baldi M, Pignatti E, Corneli G, Ghigo E, Aimaretti G, Carani C, Rochira V (2008) A novel mutation in the human aromatase gene: insights on the relationship among serum estradiol, longitudinal growth and bone mineral density in an adult man under estrogen replacement treatment. Bone 43(3):628–635. doi:10.1016/j.bone.2008.05.011
Vandenput L, Ohlsson C (2010) Sex steroid metabolism in the regulation of bone health in men. J Steroid Biochem Mol Biol 121(3–5):582–588. doi:10.1016/j.jsbmb.2010.03.067
Kelly PJ, Twomey L, Sambrook PN, Eisman JA (1990) Sex differences in peak adult bone mineral density. J Bone Miner Res 5(11):1169–1175. doi:10.1002/jbmr.5650051112
Looker AC, Wahner HW, Dunn WL, Calvo MS, Harris TB, Heyse SP, Johnston CC Jr, Lindsay R (1998) Updated data on proximal femur bone mineral levels of US adults. Osteoporos Int 8(5):468–489
WHO (2004) WHO scientific group on the assessment of osteoporosis at primary health care level
Rochira V, Faustini-Fustini M, Balestrieri A, Carani C (2000) Estrogen replacement therapy in a man with congenital aromatase deficiency: effects of different doses of transdermal estradiol on bone mineral density and hormonal parameters. J Clin Endocrinol Metab 85(5):1841–1845. doi:10.1210/jcem.85.5.6583
Bhasin S, Cunningham GR, Hayes FJ, Matsumoto AM, Snyder PJ, Swerdloff RS, Montori VM (2010) Testosterone therapy in men with androgen deficiency syndromes: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 95(6):2536–2559. doi:10.1210/jc.2009-2354
Rochira V, Santi D, Carani C (2012) Pathophysiology of estrogen action in men. In: Nieschlag E, Behre HM (eds) Testosterone. 4th edn., Cambridge University Press, pp 421–436
Khosla S, Oursler MJ, Monroe DG (2012) Estrogen and the skeleton. Trends Endocrinol Metab 23(11):576–581. doi:10.1016/j.tem.2012.03.008
Vanderschueren D, Laurent MR, Claessens F, Gielen E, Lagerquist MK, Vandenput L, Borjesson AE, Ohlsson C (2014) Sex steroid actions in male bone. Endocr Rev 35(6):906–960. doi:10.1210/er.2014-1024
Casado JL, Banon S, Andres R, Perez-Elias MJ, Moreno A, Moreno S (2014) Prevalence of causes of secondary osteoporosis and contribution to lower bone mineral density in HIV-infected patients. Osteoporos Int 25(3):1071–1079. doi:10.1007/s00198-013-2506-3
Pepe J, Isidori AM, Falciano M, Iaiani G, Salotti A, Diacinti D, Del Fiacco R, Sbardella E, Cipriani C, Piemonte S, Romagnoli E, Lenzi A, Minisola S (2012) The combination of FRAX and ageing male symptoms scale better identifies treated HIV males at risk for major fracture. Clin Endocrinol (Oxf) 77(5):672–678. doi:10.1111/j.1365-2265.2012.04452.x
Pepe J, Isidori AM, Falciano M, Iaiani G, Salotti A, Diacinti D, Del Fiacco R, Sbardella E, Cipriani C, Piemonte S, Raimo O, Biondi P, Biamonte F, Lenzi A, Minisola S (2014) Effect of risedronate in osteoporotic HIV males, according to gonadal status: a pilot study. Endocrine 47(2):456–462. doi:10.1007/s12020-014-0349-0
Trabado S, Maione L, Salenave S, Baron S, Galland F, Bry-Gauillard H, Guiochon-Mantel A, Chanson P, Pitteloud N, Sinisi AA, Brailly-Tabard S, Young J (2011) Estradiol levels in men with congenital hypogonadotropic hypogonadism and the effects of different modalities of hormonal treatment. Fertil Steril 95(7):2324–2329. doi:10.1016/j.fertnstert.2011.03.091, 2329 e2321-2323
Zirilli L, Orlando G, Carli F, Madeo B, Cocchi S, Diazzi C, Carani C, Guaraldi G, Rochira V (2012) GH response to GHRH plus arginine is impaired in lipoatrophic women with human immunodeficiency virus compared with controls. Eur J Endocrinol 166(3):415–424. doi:10.1530/eje-11-0829
Brigante G, Diazzi C, Ansaloni A, Zirilli L, Orlando G, Guaraldi G, Rochira V (2014) Gender differences in GH response to GHRH + ARG in lipodystrophic patients with HIV: a key role for body fat distribution. Eur J Endocrinol 170(5):685–696. doi:10.1530/eje-13-0961
Zona S, Guaraldi G, Luzi K, Beggi M, Santi D, Stentarelli C, Madeo B, Rochira V (2012) Erectile dysfunction is more common in young to middle-aged HIV-infected men than in HIV-uninfected men. J Sex Med 9(7):1923–1930. doi:10.1111/j.1743-6109.2012.02750.x
Santi D, Brigante G, Zona S, Guaraldi G, Rochira V (2014) Male sexual dysfunction and HIV—a clinical perspective. Nat Rev Urol 11(2):99–109. doi:10.1038/nrurol.2013.314
Martin J, Volberding P (2010) HIV and premature aging: a field still in its infancy. Ann Intern Med 153(7):477–479. doi:10.7326/0003-4819-153-7-201010050-00013
Yin MT, Zhang CA, McMahon DJ, Ferris DC, Irani D, Colon I, Cremers S, Shane E (2012) Higher rates of bone loss in postmenopausal HIV-infected women: a longitudinal study. J Clin Endocrinol Metab 97(2):554–562. doi:10.1210/jc.2011-2197
Mueller NJ, Fux CA, Ledergerber B, Elzi L, Schmid P, Dang T, Magenta L, Calmy A, Vergopoulos A, Bischoff-Ferrari HA (2010) High prevalence of severe vitamin D deficiency in combined antiretroviral therapy-naive and successfully treated Swiss HIV patients. AIDS 24(8):1127–1134. doi:10.1097/QAD.0b013e328337b161
Vescini F, Cozzi-Lepri A, Borderi M, Re MC, Maggiolo F, De Luca A, Cassola G, Vullo V, Carosi G, Antinori A, Tozzi V, Monforte AD (2011) Prevalence of hypovitaminosis D and factors associated with vitamin D deficiency and morbidity among HIV-infected patients enrolled in a large Italian cohort. J Acquir Immune Defic Syndr 58(2):163–172. doi:10.1097/QAI.0b013e31822e57e9
Moreno-Perez O, Escoin C, Serna-Candel C, Portilla J, Boix V, Alfayate R, Gonzalez-Sanchez V, Mauri M, Sanchez-Paya J, Pico A (2010) The determination of total testosterone and free testosterone (RIA) are not applicable to the evaluation of gonadal function in HIV-infected males. J Sex Med 7(8):2873–2883. doi:10.1111/j.1743-6109.2010.01886.x
Monroe AK, Brown TT (2014) Free testosterone for hypogonadism assessment in HIV-infected men. Clin Infect Dis 58(11):1640. doi:10.1093/cid/ciu129
LeBlanc ES, Nielson CM, Marshall LM, Lapidus JA, Barrett-Connor E, Ensrud KE, Hoffman AR, Laughlin G, Ohlsson C, Orwoll ES (2009) The effects of serum testosterone, estradiol, and sex hormone binding globulin levels on fracture risk in older men. J Clin Endocrinol Metab 94(9):3337–3346. doi:10.1210/jc.2009-0206
Acknowledgments
The authors thank Prof. Paola Ugolini, Department of Romance Languages, SUNY Buffalo, NY, USA for having proofread the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Rights and permissions
About this article

Cite this article
Santi, D., Madeo, B., Carli, F. et al. Serum total estradiol, but not testosterone is associated with reduced bone mineral density (BMD) in HIV-infected men: a cross-sectional, observational study. Osteoporos Int 27, 1103–1114 (2016). https://doi.org/10.1007/s00198-015-3383-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-015-3383-8