
Abstract
Summary
This study of changes in dual energy x-ray absorptiometry (DXA) spine BMD following diagnosis and treatment for childhood Crohn’s disease demonstrated that changes in conventional posteroanterior BMD results were confounded by impaired growth, and suggested that lateral spine measurements and strategies to estimate volumetric BMD were more sensitive to disease and treatment effects.
Introduction
We previously reported significant increases in peripheral quantitative CT (pQCT) measures of trabecular volumetric bone mineral density (vBMD) following diagnosis and treatment of pediatric Crohn’s disease (CD). The objective of this study was to compare pQCT trabecular vBMD and three DXA measures of spine BMD in this cohort: (1) conventional posteroanterior BMD (PA-BMD), (2) PA-BMD adjusted for height Z (PA-BMDHtZ), and (3) width-adjusted volumetric BMD (WA-BMD) estimated from PA and lateral scans.
Methods
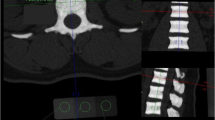
Spine DXA [lumbar (L1–4) for posteroanterior and L3 for lateral] and tibia pQCT scans were obtained in 65 CD subjects (ages 7–18 years) at diagnosis and 12 months later. BMD results were converted to sex, race, and age-specific Z-scores based on reference data in >650 children (ages 5–21 years). Multivariable linear regression models identified factors associated with BMD Z-scores.
Results
At CD diagnosis, all BMD Z-scores were lower compared with the reference children (all p values <0.01). The pQCT vBMD Z-scores (−1.46 ± 1.30) were lower compared with DXA PA-BMD (−0.75 ± 0.98), PA-BMDHtZ (−0.53 ± 0.87), and WA-BMD (−0.61 ± 1.10) among CD participants. Only PA-BMD Z-scores were correlated with height Z-scores at baseline (R = 0.47, p < 0.0001). pQCT and WA-BMD Z-scores increased significantly over 12 months to −1.04 ± 1.26 and −0.20 ± 1.14, respectively. Changes in all four BMD Z-scores were positively associated with changes in height Z-scores (p < 0.05). Glucocorticoid doses were inversely associated with changes in WA-BMD (p < 0.01) only.
Conclusions
Conventional and height Z-score-adjusted PA DXA methods did not demonstrate the significant increases in trabecular vBMD noted on pQCT and WA-BMD scans. WA-BMD captured glucocorticoid effects, potentially due to isolation of the vertebral body on the lateral projection. Future studies are needed to identify the BMD measure that provides greatest fracture discrimination in CD.
Similar content being viewed by others

References
Burnham JM, Shults J, Semeao E, Foster BJ, Zemel BS, Stallings VA, Leonard MB (2005) Body-composition alterations consistent with cachexia in children and young adults with Crohn disease. Am J Clin Nutr 82:413–420
Thayu M, Denson LA, Shults J, Zemel BS, Burnham JM, Baldassano RN, Howard KM, Ryan A, Leonard MB (2010) Determinants of changes in linear growth and body composition in incident pediatric Crohn's disease. Gastroenterology 139:430–438
Gilbert L, He X, Farmer P, Boden S, Kozlowski M, Rubin J, Nanes MS (2000) Inhibition of osteoblast differentiation by tumor necrosis factor-alpha. Endocrinology 141:3956–3964
Sylvester FA, Wyzga N, Hyams JS, Gronowicz GA (2002) Effect of Crohn’s disease on bone metabolism in vitro: a role for interleukin-6. J Bone Miner Res 17:695–702
Dalle Carbonare L, Arlot ME, Chavassieux PM, Roux JP, Portero NR, Meunier PJ (2001) Comparison of trabecular bone microarchitecture and remodeling in glucocorticoid-induced and postmenopausal osteoporosis. J Bone Miner Res 16:97–103
Canalis E, Mazziotti G, Giustina A, Bilezikian JP (2007) Glucocorticoid-induced osteoporosis: pathophysiology and therapy. Osteoporos Int 18:1319–1328
Oostlander AE, Bravenboer N, Sohl E et al (2011) Histomorphometric analysis reveals reduced bone mass and bone formation in patients with quiescent Crohn’s disease. Gastroenterology 140:116–123
Bishop N, Braillon P, Burnham J et al (2008) Dual-energy X-ray aborptiometry assessment in children and adolescents with diseases that may affect the skeleton: the 2007 ISCD Pediatric Official Positions. J Clin Densitom 11:29–42
Burnham JM, Shults J, Petit MA, Semeao E, Beck TJ, Zemel BS, Leonard MB (2007) Alterations in proximal femur geometry in children treated with glucocorticoids for Crohn disease or nephrotic syndrome: impact of the underlying disease. J Bone Miner Res 22:551–559
Burnham JM, Shults J, Semeao E, Foster B, Zemel BS, Stallings VA, Leonard MB (2004) Whole body BMC in pediatric Crohn disease: independent effects of altered growth, maturation, and body composition. J Bone Miner Res 19:1961–1968
Ahmed SF, Horrocks IA, Patterson T, Zaidi S, Ling SC, McGrogan P, Weaver LT (2004) Bone mineral assessment by dual energy X-ray absorptiometry in children with inflammatory bowel disease: evaluation by age or bone area. J Pediatr Gastroenterol Nutr 38:276–280
Harpavat M, Greenspan SL, O'Brien C, Chang CC, Bowen A, Keljo DJ (2005) Altered bone mass in children at diagnosis of Crohn disease: a pilot study. J Pediatr Gastroenterol Nutr 40:295–300
Hill RJ, Brookes DS, Lewindon PJ, Withers GD, Ee LC, Connor FL, Cleghorn GJ, Davies PS (2009) Bone health in children with inflammatory bowel disease: adjusting for bone age. J Pediatr Gastroenterol Nutr 48:538–543
Sylvester FA, Wyzga N, Hyams JS, Davis PM, Lerer T, Vance K, Hawker G, Griffiths AM (2007) Natural history of bone metabolism and bone mineral density in children with inflammatory bowel disease. Inflamm Bowel Dis 13:42–50
Walther F, Fusch C, Radke M, Beckert S, Findeisen A (2006) Osteoporosis in pediatric patients suffering from chronic inflammatory bowel disease with and without steroid treatment. J Pediatr Gastroenterol Nutr 43:42–51
Wetzsteon RJ, Petit MA, Macdonald HM, Hughes JM, Beck TJ, McKay HA (2008) Bone structure and volumetric BMD in overweight children: a longitudinal study. J Bone Miner Res 23:1946–1953
Zemel BS, Leonard MB, Kelly A et al (2010) Height adjustment in assessing dual energy x-ray absorptiometry measurements of bone mass and density in children. J Clin Endocrinol Metab 95:1265–1273
Wren TA, Liu X, Pitukcheewanont P, Gilsanz V (2005) Bone densitometry in pediatric populations: discrepancies in the diagnosis of osteoporosis by DXA and CT. J Pediatr 146:776–779
Gordon CM, Bachrach LK, Carpenter TO et al (2008) Dual energy X-ray absorptiometry interpretation and reporting in children and adolescents: the 2007 ISCD Pediatric Official Positions. J Clin Densitom 11:43–58
Leonard MB, Shults J, Zemel BS (2006) DXA estimates of vertebral volumetric bone mineral density in children: potential advantages of paired posteroanterior and lateral scans. J Clin Densitom 9:265–273
Dubner SE, Shults J, Leonard MB, Zemel BS, Sembhi H, Burnham JM (2008) Assessment of spine bone mineral density in juvenile idiopathic arthritis: impact of scan projection. J Clin Densitom 11:302–308
Liu D, Manske SL, Kontulainen SA, Tang C, Guy P, Oxland TR, McKay HA (2007) Tibial geometry is associated with failure load ex vivo: a MRI, pQCT and DXA study. Osteoporos Int 18:991–997
Dubner SE, Shults J, Baldassano RN, Zemel BS, Thayu M, Burnham JM, Herskovitz RM, Howard KM, Leonard MB (2009) Longitudinal assessment of bone density and structure in an incident cohort of children with Crohn’s disease. Gastroenterology 136:123–130
Leonard MB, Elmi A, Mostoufi-Moab S, Shults J, Burnham JM, Thayu M, Kibe L, Wetzsteon RJ, Zemel BS (2010) Effects of sex, race, and puberty on cortical bone and the functional muscle bone unit in children, adolescents, and young adults. J Clin Endocrinol Metab 95:1681–1689
Hyams JS, Ferry GD, Mandel FS et al (1991) Development and validation of a pediatric Crohn’s disease activity index. J Pediatr Gastroenterol Nutr 12:439–447
Schall JI, Semeao EJ, Stallings VA, Zemel BS (2002) Self-assessment of sexual maturity status in children with Crohn’s disease. J Pediatr 141:223–229
Tanner JM (1962) Growth at adolescence. Blackwell Scientific Publication, Oxford, United Kingdom
Blake GM, Jagathesan T, Herd RJ, Fogelman I (1994) Dual X-ray absorptiometry of the lumbar spine: the precision of paired anteroposterior/lateral studies. Br J Radiol 67:624–630
Ogden CL, Kuczmarski RJ, Flegal KM, Mei Z, Guo S, Wei R, Grummer-Strawn LM, Curtin LR, Roche AF, Johnson CL (2002) Centers for Disease Control and Prevention 2000 growth charts for the United States: improvements to the 1977 National Center for Health Statistics version. Pediatrics 109:45–60
Cole TJ (1990) The LMS method for constructing normalized growth standards. Eur J Clin Nutr 44:45–60
Andres PG, Friedman LS (1999) Epidemiology and the natural course of inflammatory bowel disease. Gastroenterol Clin N Am 28:255–281, vii
Gupta A, Paski S, Issenman R, Webber C (2004) Lumbar spine bone mineral density at diagnosis and during follow-up in children with IBD. J Clin Densitom 7:290–295
Wetzsteon RJ, Shults J, Zemel BS, Gupta PU, Burnham JM, Herskovitz RM, Howard KM, Leonard MB (2009) Divergent effects of glucocorticoids on cortical and trabecular compartment BMD in childhood nephrotic syndrome. J Bone Miner Res 24:503–513
Thearle M, Horlick M, Bilezikian JP, Levy J, Gertner JM, Levine LS, Harbison M, Berdon W, Oberfield SE (2000) Osteoporosis: an unusual presentation of childhood Crohn’s disease. J Clin Endocrinol Metab 85:2122–2126
Lee DC, Gilsanz V, Wren TA (2007) Limitations of peripheral quantitative computed tomography metaphyseal bone density measurements. J Clin Endocrinol Metab 92:4248–4253
Yu W, Gluer CC, Grampp S, Jergas M, Fuerst T, Wu CY, Lu Y, Fan B, Genant HK (1995) Spinal bone mineral assessment in postmenopausal women: a comparison between dual X-ray absorptiometry and quantitative computed tomography. Osteoporos Int 5:433–439
Finkelstein JS, Cleary RL, Butler JP, Antonelli R, Mitlak BH, Deraska DJ, Zamora-Quezada JC, Neer RM (1994) A comparison of lateral versus anterior-posterior spine dual energy x-ray absorptiometry for the diagnosis of osteopenia. J Clin Endocrinol Metab 78:724–730
Laakso S, Valta H, Verkasalo M, Toiviainen-Salo S, Viljakainen H, Makitie O (2012) Impaired bone health in inflammatory bowel disease: a case–control study in 80 pediatric patients. Calcif Tissue Int 91:121–130
Tsampalieros A, Griffin L, Terpstra AM, Kalkwarf H, Shults J, Foster BJ, Zemel BS, Foerster D, Leonard MB (2013 in press) DXA measures of disease and treatment effects on bone mass and body composition after pediatric renal transplantation. Am J Transplant
Wren TA, Shepherd JA, Kalkwarf HJ, Zemel BS, Lappe JM, Oberfield S, Dorey FJ, Winer KK, Gilsanz V (2012) Racial disparity in fracture risk between white and nonwhite children in the United States. J Pediatr 161:1035–1040
Kalkwarf HJ, Laor T, Bean JA (2011) Fracture risk in children with a forearm injury is associated with volumetric bone density and cortical area (by peripheral QCT) and areal bone density (by DXA). Osteoporos Int 22:607–616
Makitie O, Doria AS, Henriques F, Cole WG, Compeyrot S, Silverman E, Laxer R, Daneman A, Sochett EB (2005) Radiographic vertebral morphology: a diagnostic tool in pediatric osteoporosis. J Pediatr 146:395–401
Rodd C, Lang B, Ramsay T et al (2012) Incident vertebral fractures among children with rheumatic disorders 12 months after glucocorticoid initiation: a national observational study. Arthritis Care Res 64:122–131
Acknowledgments
We greatly thank the children and their families who participated in this study for their dedication and the physicians and nurses in the Division of Gastroenterology at the Children’s Hospital of Philadelphia. This project was supported by grants R01-DK060030, K24-DK076808, and UL1-RR-024134 from the National Center for Research Resources. Dr. Berkenstock was supported by the Society of Pediatric Research, Dr. Tsampalieros by the University of Ottawa, Faculty of Medicine, and Dr. Griffin by the Doris Duke Clinical Research Foundation.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Tsampalieros, A., Berkenstock, M.K., Zemel, B.S. et al. Changes in trabecular bone density in incident pediatric Crohn’s disease: a comparison of imaging methods. Osteoporos Int 25, 1875–1883 (2014). https://doi.org/10.1007/s00198-014-2701-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-014-2701-x