
Abstract
Introduction and hypothesis
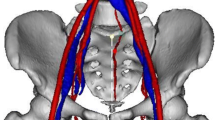
Pelvic anatomy is complex and intimate knowledge of variabilities in anatomical relationships is critical for surgeons to safely perform surgical procedures. Three-dimensional Imaging provides the opportunity to analyze undisturbed anatomical relationships. The authors hypothesized that three-dimensional models created from pelvic computed tomography angiograms could be used to obtain vascular anatomical measurements, and that the measurements obtained from three-dimensional models would be similar to those from cadaver studies.
Methods
We included all pelvic computed tomography angiograms that were acquired in female patients older than 18 years at our institution within the previous 5 years. Three-dimensional models were created using the Invivo5 software based on the Digital Imaging and Communications in Medicine files. Structures of interest were virtually dissected and measured replicating previous cadaver studies. Statistical analysis of demographics and measurements was performed.
Results
The final analysis included 87 studies. The average age of the subjects was 66.9 years and their average BMI was 26.1 kg/m2. Of the 87 subjects, 12.6% had a history of hysterectomy, 2.3% a history of a continence procedure, and 1.1% a history of a prolapse procedure. The range of distance between the ischial spine and the pudendal artery was 3–17 mm. The closest vessels to the lower edge of the symphysis pubis were the obturator vessels. The aberrant corona mortis vessel was present in 27.9% of the subjects. Prior hysterectomy was associated with changes in the measurements of the obturator arteries with minimal changes in other measurements.
Conclusions
Our results indicate that this technology provides similar measurements to those found in previous unembalmed cadaver studies. This technology offers a great opportunity to study anatomical relationships in a native undisturbed state.



Similar content being viewed by others

References
Mitsiopoulos N, Baumgartner RN, Heymsfield SB, Lyons W, Gallagher D, Ross R. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J Appl Physiol (1985). 1998;85:115–122.
ElKhamary SM, Riad W. Three dimensional MRI study: safety of short versus long needle peribulbar anesthesia. Saudi J Ophthalmol. 2014;28:220–224.
Good MM, Abele TA, Balgobin S, Schaffer JI, Slocum P, McIntire D, et al. Preventing L5-S1 discitis associated with sacrocolpopexy. Obstet Gynecol. 2013;121:285–290.
Pizzoferrato AC, Nyangoh Timoh K, Fritel X, Zareski E, Bader G, Fauconnier A. Dynamic magnetic resonance imaging and pelvic floor disorders: how and when? Eur J Obstet Gynecol Reprod Biol. 2014;181:259–266.
Varkarakis J, Sebe P, Pinggera GM, Bartsch G, Strasser H. Three-dimensional ultrasound guidance for percutaneous drainage of prostatic abscesses. Urology. 2004;63:1017–1020. discussion 1020.
Thompson JR, Gibb JS, Genadry R, Burrows L, Lambrou N, Buller JL. Anatomy of pelvic arteries adjacent to the sacrospinous ligament: importance of the coccygeal branch of the inferior gluteal artery. Obstet Gynecol. 1999;94:973–977.
Muir TW, Tulikangas PK, Fidela Paraiso M, Walters MD. The relationship of tension-free vaginal tape insertion and the vascular anatomy. Obstet Gynecol. 2003;101:933–936.
Ates M, Kinaci E, Kose E, Soyer V, Sarici B, Cuglan S, et al. Corona mortis: in vivo anatomical knowledge and the risk of injury in totally extraperitoneal inguinal hernia repair. Hernia. 2016;20:659–665.
Stavropoulou-Deli A, Anagnostopoulou S. Corona mortis: anatomical data and clinical considerations. Aust N Z J Obstet Gynaecol. 2013;53:283–286.
Eisma R, Wilkinson T. From “silent teachers” to models. PLoS Biol. 2014;12, e1001971.
Trelles M, Eberhardt KM, Buchholz M, Schindler A, Bayer-Karpinska A, Dichgans M, et al. CTA for screening of complicated atherosclerotic carotid plaque – American Heart Association type VI lesions as defined by MRI. AJNR Am J Neuroradiol. 2013;34:2331–2337.
Barksdale PA, Elkins TE, Sanders CK, Jaramillo FE, Gasser RF. An anatomic approach to pelvic hemorrhage during sacrospinous ligament fixation of the vaginal vault. Obstet Gynecol. 1998;91:715–718.
Roshanravan SM, Wieslander CK, Schaffer JI, Corton MM. Neurovascular anatomy of the sacrospinous ligament region in female cadavers: implications in sacrospinous ligament fixation. Am J Obstet Gynecol. 2007;197:660.e1–660.e6.
Sivanesan K, Abdel-Fattah M, Ghani R. External iliac artery injury during insertion of tension-free vaginal tape: a case report and literature review. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18:1105–1108.
Rehder P, Glodny B, Pichler R, Mitterberger MJ. Massive retropubic hematoma after minimal invasive mid-urethral sling procedure in a patient with a corona mortis. Indian J Urol. 2010;26:577–579.
Gobrecht U, Kuhn A, Fellman B. Injury of the corona mortis during vaginal tape insertion (TVT-Secur using the U-Approach). Int Urogynecol J. 2011;22:443–445.
Drewes PG, Marinis SI, Schaffer JI, Boreham MK, Corton MM. Vascular anatomy over the superior pubic rami in female cadavers. Am J Obstet Gynecol. 2005;193:2165–2168.
Acknowledgements
We acknowledge the support of the Interprofessional Center for Experiential Learning and Simulation (iCELS) of the University of Massachusetts Medical School in facilitating access to and use of the Invivo5 software.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Rights and permissions
About this article

Cite this article
Dueñas-Garcia, O.F., Kim, Y., Leung, K. et al. Vascular anatomical relationships of the retropubic space and the sacrospinous ligament, using three-dimensional imaging. Int Urogynecol J 28, 1177–1182 (2017). https://doi.org/10.1007/s00192-016-3240-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-016-3240-0