
Abstract
Introduction and hypothesis
Intra-vaginal diazepam suppositories are commonly prescribed as a treatment option for high-tone pelvic floor myalgia. This triple-blinded placebo-controlled randomized trial sought to determine if 10 mg diazepam suppositories improve resting pelvic floor electromyography (EMG) compared with placebo.
Methods
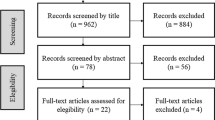
Women ≥18 years of age with hypertonic pelvic floor muscles on examination, confirmed by resting EMG ≥2.0 microvolts (μv), administered vaginal suppositories containing either diazepam or placebo for 28 consecutive nights. Outcomes included vaginal surface EMG (four measurements), the Female Sexual Function Index (FSFI), the Short Form Health Survey 12 (SF-12), four visual analog scales (VAS), the Patient Global Impression of Severity (PGI-S), and the Patient Global Impression of Improvement (PGI-I). A priori sample size calculation indicated that 7 subjects in each group could detect a 2-μv difference in resting EMG tone with 90 % power.
Results
Twenty-one subjects were enrolled. The mean age was 36.1 (SD 13.9) years, mean body mass index was 28.56 (SD 9.4), and the majority (85.7 %) was Caucasian. When evaluating response to therapy, no difference was seen in any of the resting vaginal EMG assessments at any time point within subjects or between groups, nor was an interaction found. Additionally, no differences were noted in any of the validated questionnaires.
Conclusions
When used nightly over 4 weeks, 10 mg of vaginal diazepam was not associated with improvement in resting EMG parameters or subjective outcomes compared with placebo. This suggests such that therapy alone may be insufficient in treating high-tone pelvic floor dysfunction.



Similar content being viewed by others


References
Rogalski MJ, Kellog-Spadt S, Hoffmann AR, Fariello JY, Whitmore KE (2010) Retrospective chart review of vaginal diazepam suppository use in high-tone pelvic floor dysfunction. Int Urogynecol J 21:895–899
Lukban J, Whitmore K, Kellog-Spadt S, Bologna R, Lesher A, Fletcher E (2001) The effect of manual physical therapy in patients diagnosed with interstitial cystitis, high-tone pelvic floor dysfunction, and sacroiliac dysfunction. Urology 57 [6 Suppl 1]:121–122
Oyama IA, Rejba A, Lubkan JC, Fletcher E, Kellog-Spadt S, Holzberg AS, Whitmore KE (2004) Modified Thiele massage as therapeutic intervention for female patients with interstitial cystitis and high-tone pelvic floor dysfunction. Urology 64:862–865
Ger GC, Wexner SD, Jorge JM, Salanga VD (1993) Anorectal manometry in the diagnosis of paradoxical puborectalis syndrome. Dis Colon Rectum 36:816–825
Rapkin AJ, Kames LD (1987) The pain management approach to chronic pelvic pain. J Reprod Med 32:323–327
Srinivasan AK, Kaye JD, Moldwin R (2007) Myofascial dysfunction associated with chronic pelvic floor pain: management strategies. Curr Pain Headache Rep 11:359–364
Wiegel M, Meston C, Rosen R (2005) The female sexual function index (FSFI): cross-validation and development of clinical cutoff scores. J Sex Marital Ther 31:1–20
Ware J Jr, Kosinski M, Keller SD (1996) A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care 34:220–233
Von Korff M, Deyo RA, Cherkin D, Barlow W (1993) Back pain in primary care. Outcomes at 1 year. Spine (Phila Pa 1976) 18:855–862
Yalcin I, Bump RC (2003) Validation of two global impression questionnaires for incontinence. Am J Obstet Gynecol 189:98–101
Srikrishna S, Robinson D, Cardozo L (2010) Validation of the Patient Global Impression of Improvement (PGI-I) for urogenital prolapse. Int Urogynecol J 21:523–528
Kotarinos RK (2003) Pelvic floor physical therapy in urogynecologic disorders. Curr Womens Health Rep 3:334–339
Glazer HI, Jantos M, Hartmann EH, Swencionis C (1998) Electromyographic comparisons of the pelvic floor in women with dysesthetic vulvodynia and asymptomatic women. J Reprod Med 43:959–962
White G, Jantos M, Glazer H (1997) Establishing the diagnosis of vulvar vestibulitis. J Reprod Med 42:157–160
Wehbe SA, Whitmore K, Kellogg-Spadt S (2010) Urogenital complaints and female sexual dysfunction (part 1). J Sex Med 7:1704–1713, quiz 1703, 1714–1715
Thiele GH (1963) Coccygodynia: cause and treatment. Dis Colon Rectum 6:422–436
Langford CF, Udvari Nagy S, Ghoniem GM (2007) Levator ani trigger point injections: an underutilized treatment for chronic pelvic pain. Neurourol Urodyn 26:59–62
Cram JR (1998) Cram’s introduction to surface electromyography. Jones and Bartlett, Sudbury
Acknowledgements
The authors would like to thank Vivian Ghodsi RN, CCRC, for her valuable help with patient screening, data collection, and subject follow-up for this study.
Funding
This study was funded by an education grant through the TriHealth Medical Education Research Fund.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Crisp, C.C., Vaccaro, C.M., Estanol, M.V. et al. Intra-vaginal diazepam for high-tone pelvic floor dysfunction: a randomized placebo-controlled trial. Int Urogynecol J 24, 1915–1923 (2013). https://doi.org/10.1007/s00192-013-2108-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-013-2108-9