
Abstract
Introduction and hypothesis
The aim of this study was to compare outcome and quality of life of tension-free vaginal tape “inside-out” (TVT-O) and Monarc transobturator tapes after 2–4 years.
Methods
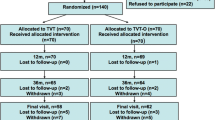
The method used was a prospective comparative study. Participants (n = 191) were assigned to either a TVT-O (n = 93) or a Monarc (n = 98) procedure. Cure of stress urinary incontinence (SUI) was defined as the statement of the woman of not experiencing any loss of urine upon physical exercise.
Results
Cure rates after 2–4 years were 72% for TVT-O and 65% for Monarc, while improvement was observed in, respectively, 12% and 21% (p = 0.3). There was a statistically significant improvement in quality of life but no differences were found between both procedures.
Conclusions
After a 2–4-year follow-up period, both procedures were equally safe and effective in curing SUI.
Similar content being viewed by others


Introduction
Until recently, the Burch colposuspension was the standard procedure for the treatment of female stress urinary incontinence (SUI) [1, 2]. Since its introduction in 1995, tension-free vaginal tape (TVT) became the new “gold” standard in the surgical treatment of SUI. TVT has been proven to be as effective as the Burch colposuspension with success rates ranging from 84% to 95%, but has less side effects and complications [3-5]. In 2001, Delorme introduced transobturator tape (TOT) with a high success rate [6]. This sling is also located underneath the mid-urethra, but runs laterally through the obturator membrane to the upper part of the thigh.
There are two basic techniques for performing TOT: “outside-in” described by Delorme [6] and “inside-out” (TVT-O) described by de Leval [7]. These techniques differ not only in the way the needle is placed and carried forward but also in the different designs of the introducer. After the introduction of the outside-in technique by Delorme in 2001, several other similar procedures were developed. Among them is Monarc, which consists like TVT-O of a monofilament macroporous polypropylene mesh and which has shown similar and equally good short- to medium-term success rates as TVT-O [8, 9].
However, until now, there is little evidence that one technique is superior to the other. Furthermore, no comparative trials are published with follow-up longer than 1 year. Therefore, the aim of this study is to compare the outcome and the quality of life results of two existing different TOT procedures inside-out (TVT-O) and outside-in (Monarc) for the treatment of SUI after a 2–4-year follow-up.
Materials and methods
Between October 2004 and December 2006, 191 consecutive women with an indication for surgical treatment of SUI underwent either the TVT-O or the Monarc procedure. This study was approved by the Medical Ethical Committee of the St. Elisabeth Hospital as part of a multicentre study on the outcome of transobturator tape as treatment for predominant female SUI.
Included were 93 women with a TVT-O and 98 women with a Monarc procedure. Women who did not show up for their 2–4-year follow-up visit first received a questionnaire and, if they did not reply, were later contacted by one of the investigators (MH).
Excluded were women with recurrent and difficult to treat urinary tract infections, significant and predominantly symptoms of urge urinary incontinence, post voiding bladder retention of more than 150 ml, bladder capacity of less than 100 ml, and physical or mental impairment to adequately register outcome results or complications.
A standardized urogynecological history and physical examination was performed preoperative, after 2 months, 1 year, and after 2 to 4 years. Preoperative multichannel urodynamic investigation was carried in all women according to the International Continence Society standards [10, 11].
All women were asked to complete the short version of the Incontinence Impact Questionnaire (IIQ-7) and the Urogenital Distress Inventory (UDI-6) before and at the above-mentioned postoperative intervals. These questionnaires are internationally accepted as valid disease-specific quality of life (QoL) instruments and are sensitive to change [12]. They have been translated into Dutch language and validated [13]. The questionnaires were anonymously entered in a database, and researchers were blinded to the individual results of these questionnaires. The total score of the IIQ-7 and UDI-6 was transformed to a scale from 0 to 100 (a higher score indicates more bother).
Women were assigned to either a TVT-O or a Monarc procedure just before surgery was to take place. The inside-out procedure was performed as described by de Leval [7], and a TVT-O (Gynecare, Sommerville, NJ, USA) tape was inserted. The Monarc (American Medical Systems, Minneapolis, MN, USA) tape was inserted through the outside-in route as using the technique recommended by the manufacturer. Both procedures use a monofilament, macroporous polypropylene tape, which is placed under the urethra without any tension. Surgery was not accompanied by other urogynecological procedures.
All procedures were carried out under general anesthesia, and hence, no intra-operative cough stress test was performed. Cystoscopy was performed only in case of encountering bloody urine. All women received preoperative antibiotics, and this was continued for 7 days postoperative. All procedures were performed in the St. Elisabeth Hospital Tilburg, The Netherlands.
We adhered to the recommendations of IUGA on outcome measures [14]. Cure of SUI was defined as the statement of the woman of not experiencing any loss of urine upon physical exercise. Other definitions in this study are in accordance with the terminology of the International Continence Society [10].
Continuous variables were compared using unpaired t test, and dichotomous variables were compared using chi-square test. Fisher’s exact test was used if cross tabs had a cell with an expected frequency <5. The minimum level of significance was 0.05. Statistical analyses were performed with SPSS (Windows version 16.0).
Results
After a 2–4-year follow-up, 161 (84%) women were available for evaluation. The TVT-O group consisted of 75 women compared to 86 women in the Monarc group. The mean follow-up of the TVT-O group was 38 months (range 12–53 months) and 39 months (range 12–53 months) in the Monarc group. For their 2–4-year follow-up control, 76 (47%) women visited our outpatient department, 51 (32%) women answered a questionnaire by mail, and 34 (21%) women answered a telephonic questionnaire by one of the investigators (MH). The response rate of the QoL questionnaires was 92%, 81%, 81%, and 70% respectively prior to, 2 months and 1 year postoperatively, and after 2–4 years. There were no differences in method of follow-up or response rate of QoL questionnaires between both groups.
Preoperative data are listed in Table 1. No differences between both groups were observed. In women with mixed urinary incontinence (MUI), anti-cholinergic medical treatment was given before surgical treatment was considered and did not alleviate their symptoms. The majority (89%) of the women underwent preoperative pelvic floor physiotherapy.
Surgical data are depicted in Table 2. No concomitant urogynecological surgery was performed, but in 15 women (8%), surgery was combined with non-urogynecological procedures. There are no differences in surgery time, amount of blood loss, and type of anesthesia between TVT-O and Monarc.
Outcome data are presented in Table 3. The cure rate for TVT-O was 72% after 2–4 years compared to 65% in the Monarc group, while improvement was observed in respectively 12% and 21% (p = 0.3). Preexisting urge incontinence resolved in seven women (32%) after TVT-O and eight women (31%) after Monarc (p = 1.0). De novo urge incontinence developed in two cases in the TVT-O group versus four cases in the Monarc group (p = 0.2).
Both the IIQ-7 and UDI-6 demonstrated a statistically significant increase in QoL decrease in impairment caused by symptoms of SUI after 2 months, 1 year, and 2–4 years in both TOT groups.
Any complications are presented in Table 4. No major intra-operative complications occurred. After 2 months, voiding difficulty was more observed in the TVT-O group. Tape release was carried out in one woman in the TVT-O group because of vaginal pain and a superficial located and palpable tape. She remained continent. In one other woman, tape release was indicated for voiding difficulty. Afterward, voiding became normal and they remained continent.
There were five cases of vaginal erosion, which were all excised under local anesthesia, and all remained continent afterward. In five women after TVT-O and in four women after Monarc, a second anti-incontinence procedure was performed (p = 0.5). As second incontinence procedures, tension-free vaginal tape (seven times), tension-free vaginal tape Secur (once), and Remeex system (once) were performed. The stress incontinence was resolved in all nine women. In one other woman, a stitch was placed under the mid-urethra under local anesthesia after which her already improved SUI disappeared.
Discussion
This report comprises a large comparative study of both procedures with the longest follow-up until now. The main objective of this study was to compare outcome and complications for an inside-out versus an outside-in transobturator approach. The second objective was to evaluate results of both obturator approaches after a 2–4-year follow-up. We did not find significant differences between both approaches. Approximately 85% of the women found their symptoms to be improved after 2–4 years, which are satisfying results.
Most studies comparing TVT-O and Monarc have a short follow-up time and differ with respect to definitions of success. Debodinance compared 50 TVT-O procedures to 50 Monarc procedures in a prospective observational study [15]. With a definition of cure as being continent at postoperative urodynamic assessment, 47 (94%) women with TVT-O and 45 (90%) with Monarc were cured after 1 year. Lee et al. prospectively compared 100 women who underwent either a TVT-O (n = 50) or a TOT (Dow Medics, Korea, n = 50) procedure and defined cure as a negative cough stress test and no reports of urine leakage during stress [16]. Equal cure rates for TVT-O and TOT were found: 86% versus 92% 1 year after surgery. Liapsis et al. followed up 114 women who were prospectively randomized to TVT-O or Monarc for 1 year [17]. Cure was defined as a negative cough stress test during multichannel urodynamic investigation and a 1-h pad test giving a weight of less than 1 g. Cure rate in the TVT-O group was 87% (53 of 61 women) and 90% (48 of 53 women) in the Monarc group. Subjective cure was remarkably lower: 80% in the TVT-O group versus 77% in the Monarc group.
Not many studies have investigated the medium-term results (>1 year) of obturator tapes. Waltregny et al. followed up 91 women prospectively after a TVT-O procedure with a minimum follow-up of 3 years [18]. Cure of SUI was defined by the disappearance of subjective SUI, as assessed by a SUI symptom scale score equal to 0. Disappearance and improvement of SUI was observed in 88% and 9% of the women, respectively. Wang et al. found an 83% cure rate 36 months after a TVT-O procedure. The clinical outcome was regarded as cured when the cough test was negative at the follow-up visit. Their results were based on 30 women with a 36-month follow-up.
The above-mentioned comparative studies show as presented in this study that both TVT-O and Monarc are equally effective in curing SUI after 1 year [15-17]. On longer follow-up, our results are lower compared to the mentioned studies [18, 19]. This might be due to our definition of cure. We intentionally used the statement of women about losing urine upon physical exercise. Although this is a subjective parameter, it does give information about the experience of women over a longer period of time. This may provide more or different information than objective parameters like a postoperative stress test, pad test, or urodynamic investigation, which just reflect a measurement at one point in time. We realize however that in a small number of women it is quite possible that “failures” are actually reporting the symptom of urge incontinence rather than the diagnosis of genuine stress incontinence. To demonstrate this difference, objective testing would be required.
Our strict definition of success, being no loss of urine at all, may be unrealistic compared to the occurrence of incontinence and experience of women in the normal population. Becoming fully continent after TVT is not synonymous with being satisfied. A number of operated women still leaked postoperatively but were satisfied. These were mostly women with severe incontinence who experienced substantial improvement, the incontinence being reduced to an acceptable degree. This corroborates the finding that women can cope with a certain degree of incontinence for which therapy is not warranted [20]. However, for scientific purposes, it is perhaps better and gives accurate insight in cure and improvement rates. For counseling purposes to women, the improvement rate is also of importance. In our study with a long follow-up of 2 to 4 years, 72% of women with a TVT-O were cured and another 12% improved, while in the Monarc group, these numbers are, respectively, 65% and 21%. This indicates that most women are still much better off after these incontinence procedures.
In determining success, another important parameter is the improvement in quality of life. In our study, QoL parameters improved significantly in both groups, and no differences were found between the two procedures. In general, the improvement observed after both procedures seems comparable to QoL improvement after a TVT procedure [3].
Other functional changes are related to the development of de novo urge incontinence and voiding difficulty or the resolution of these symptoms. The risk for developing de novo urge incontinence seems to be equal after Monarc and TVT-O procedures. This observation is confirmed by the other comparative studies [15-17]. The number of women reporting voiding difficulty after 2 months is higher in the TVT-O group. There is no explanation for this difference. Latthe’s results [21] indicate that voiding difficulty was less for combined TVT-O and TOT tapes compared to the retropubic TVT procedure. On subgroup analysis, they found no differences between the procedures by either obturator route.
Anatomical complications like bladder or urethra injury or bleeding of more than 300 ml did not occur in this study. Furthermore, the three remaining complications in this study (two accidental fausse routes and one premature cutting of the tape) are relative minor incidents. Both TVT-O and Monarc have substantial lower intra-operative complication rates than TVT, but no differences between both procedures are observed [21].
When TVT-O and Monarc became available, there was some evidence that one procedure could be less safe than the other. Achtari et al. [22] showed by cadaveric dissection that TVT-O runs more closely to the obturator canal, making TVT-O more prone to possible injury of the obturator nerve and vessels. We did not find any obturator nerve or vessel injury, and apparently, this theoretical risk does not exist in clinical practice.
Although the number of women is too small to draw conclusions, there seems to be a little higher erosion rate in the Monarc group. These results are confirmed by other publications but a significant difference was never reached, mostly due small patient numbers [21]. Nevertheless, the postoperative complication rate in our study population is low, and no differences between both procedures were observed.
Advantages of this study are the large number of women with only 16% loss to follow-up after 2–4 years. Other advantages are a strict outcome parameter, a consistent treatment strategy where procedures were not combined with other urogynecological treatments, the standardized urogynecological work-up (including urodynamic investigation), and the fact that all women were treated in one clinic by two urogynecologists and residents (always with supervision and the presence of these urogynecologist during surgery).
The draw-back of this study may be the bias in follow-up results. Not all women visited our outpatient department for the follow-up procedure. There may be a difference in the results of women visiting our outpatient department compared to women answering questionnaires by mail or telephone. Nevertheless, the use of interviews by telephone allowed us to minimize the loss to follow-up.
This study shows equal clinical cure rates and improvement in quality of life for both TVT-O and Monarc as a surgical treatment for stress urinary incontinence on the long run. Nevertheless, while longer follow-up data of TVT are now available [23], longer follow-up than 4 years is still mandatory.
References
Burch JC (1961) Urethrovaginal fixation to Cooper’s ligament for correction of stress incontinence, cystocele, and prolapse. Am J Obstet Gynecol 81:281–290
Burch JC (1968) Cooper’s ligament urethrovesical suspension for stress incontinence. Nine years’ experience--results, complications, technique. Am J Obstet Gynecol 100:764–774
Schraffordt Koops SE, Vervest HAM, Bisseling TM (2003) The outcome of TVT analysed with disease-specific quality of life questionnaires: results from the Netherlands Multicenter TVT Study. Neurourol Urodyn 22:404–405
Ward K, Hilton P (2002) Prospective multicentre randomised trial of tension-free vaginal tape and colposuspension as primary treatment for stress incontinence. BMJ 325(7355):67
Ward KL, Hilton P (2004) A prospective multicenter randomized trial of tension-free vaginal tape and colposuspension for primary urodynamic stress incontinence: two-year follow-up. Am J Obstet Gynecol 190:324–331
Delorme E (2001) Transobturator urethral suspension: mini-invasive procedure in the treatment of stress urinary incontinence in women. Prog Urol 11:1306–1313
de Leval J (2003) Novel surgical technique for the treatment of female stress urinary incontinence: transobturator vaginal tape inside-out. Eur Urol 44:724–730
Davila GW, Johnson JD, Serels S (2006) Multicenter experience with the Monarc transobturator sling system to treat stress urinary incontinence. Int Urogynecol J 17:460–465
Naidu A, Lim YN, Barry C, Goodwin S, Corstiaans A, Rane A (2005) Transobturator tape for stress incontinence: the North Queensland experience. Aust NZ J Obstet Gynaecol 45(5):446–449
Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U et al (2002) The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn 21:167–178
Schafer W, Abrams P, Liao L, Mattiasson A, Pesce F, Spangberg A et al (2002) Good urodynamic practices: uroflowmetry, filling cystometry, and pressure-flow studies. Neurourol Urodyn 21:261–274
Fitzgerald MP, Kenton K, Shott S, Brubaker L (2001) Responsiveness of quality of life measurements to change after reconstructive pelvic surgery. Am J Obstet Gynecol 185:20–24
van der Vaart CH, de L Jr, Roovers JP, Heintz AP (2003) Measuring health-related quality of life in women with urogenital dysfunction: the urogenital distress inventory and incontinence impact questionnaire revisited. Neurourol Urodyn 22:97–104
Ghoniem G, Stanford E, Kenton K, Achtari C, Goldberg R, Mascarenhas T, Parekh M et al (2008) Evaluation and outcome measures in the treatment of female urinary stress incontinence: International Urogynecological Association (IUGA) guidelines for research and clinical practice. Int Urogynecol J Pelvic Floor Dysfunct 19:5–33
Debodinance P (2007) Trans-obturator urethral sling for the surgical correction of female stress urinary incontinence: outside-in (Monarc) versus inside-out (TVT-O). Are the two ways reassuring? Eur J Obstet Gynecol Reprod Biol 133:232–238
Lee KS, Choo MS, Lee YS, Han J, Kim J, Jung BJ, Han DK (2008) Prospective comparison of the “inside-out” and “outside-in” transobturator tape procedures for the treatment of female stress urinary incontinence. Int Urogynecol J 19(4):577–582
Liapsis A, Bakas P, Creatsas G (2008) Monarc vs TVT-O for the treatment of primary stress incontinence: a rondomised study. Int Urogynecol J 19(2):185–190
Waltregny D, Gaspar Y, Reul O, Hamida W, Bonnet P, de Leval J (2008) TVT-O for the treatment of female stress urinary incontinence: results of a prospective study after a 3-year minimum follow-up. Eur Urol 53(2):401–408
Wang W, Zhu L, Lang J (2009) Transobturator tape procedure versus tension-free vaginal tape for treatment of stress urinary incontinence. Int J Gynaecol Obstet 104(2):113–116
Jolleys JV (1988) Reported prevalence of urinary incontinence in women in a general practice. Br Med J 296:1300–1302
Latthe PM, Foon R, Toozs-Hobson P (2007) Transobturator and retropubic tape procedures in stress urinary incontinence: a systematic review and meta-analysis of effectiveness and complications. BJOG 114:522–531
Achtari C, McKenzie BJ, Hiscock R, Rosamilia A, Schierlitz L, Briggs CA, Dwyer PL (2006) Anatomical study of the obturator foramen and dorsal nerve of the clitoris and their relationship to minimally invasive slings. Int Urogynecol J Pelvic Floor Dysfunct 17(4):330–334
Nilsson CG, Palva K, Rezapour M, Falconer C (2008) Eleven years prospective follow-up of the tension-free vaginal tape procedure for treatment of stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct 19(8):1043–1047
Conflicts of interest
None.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Houwert, R.M., Renes-Zijl, C., Vos, M.C. et al. TVT-O versus Monarc after a 2–4-year follow-up: a prospective comparative study. Int Urogynecol J 20, 1327–1333 (2009). https://doi.org/10.1007/s00192-009-0943-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-009-0943-5