
Abstract
Purpose
Peripheral nerve blocks can be a suitable alternative to central neuraxial blockage, as the sole anaesthetic agent for better early postoperative outcomes, decreased hospital stay and earlier mobilisation after anterior cruciate ligament reconstruction (ACLR) surgery. The purpose of this study was to compare consciousness during the procedure, pain during early postoperative period (< 7 days), and perioperative outcomes following ACLR using combined sciatic, femoral, and obturator nerve blocks compared to the spinal anaesthesia.
Methods
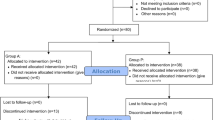
This was a prospective case–control study including patients between 18 and 55 years of age, with anterior cruciate ligament (ACL) injury confirmed clinically and radiologically and undergoing ACLR. Patients were allocated in the two groups alternatively, group 1 included patients who received combined nerve blocks, and group 2 included patients who received spinal anaesthesia for the surgery. The sensory effect, motor effect, adequacy of anaesthesia, perioperative analgesic use, duration of stay, postoperative pain (visual analogue scale 0–10 cm) and functional outcomes were noted.
Results
There were 60 patients in each group. A total of seven patients in group 1 (11%) and two patients in group 2 (3%) needed conversion to general anaesthesia (n.s.). In group 1, out of 53 patients who underwent surgery, 26 patients had no perception of surgery in the joint, 17 patients had perception of manipulation of the knee joint, 4 patients had sense of touch, and 6 patients had sensation of pain in the knee (VAS scale less than 3). In group 2, out of 58 patients, 42 patients had no perception of surgery, 12 had a perception of manipulation of the knee joint, 2 had sense of touch, and 2 had sensation of pain in the knee. Blockage of sensory effect was significantly better in group 2 (p = 0.0001). However, the motor effect was comparable between the two groups (n.s.). Group 1 had significantly better pain scores 6, 12, and 18 h after the surgery. Moreover, patients in group 1 also had faster ambulation (mean difference of 5.5 h, p = 0.0001) and reduced hospital stay (mean difference of 8.4 h, p = 0.0001).
Conclusion
Combined sciatic, femoral, and adductor canal block is an effective sole anaesthetic modality for ACLR. The sensory effect was inferior when compared to spinal anaesthesia but sufficient for the procedure without the need for supplementation with any other anaesthetic modality. Patients receiving this combined nerve block had lesser early postoperative pain scores, earlier ambulation, and shorter hospital stay as compared to the spinal anaesthesia.
Level of evidence
Level 3.
Similar content being viewed by others


References
Ambrosoli AL, Guzzetti L, Severgnini P, Fedele LL, Musella G, Crespi A et al (2019) Postoperative analgesia and early functional recovery after day-case anterior cruciate ligament reconstruction: a randomized trial on local anesthetic delivery methods for continuous infusion adductor canal block. Minerva Anestesiol 85:962–970
Bansal L, Attri J, Verma P (2016) Lower limb surgeries under combined femoral and sciatic nerve block. Anesth Essays Res 10:432
Barbier D, N’Dele D, Bennis M, Thevenin-Lemoine C, Sales De Gauzy J, Accadbled F (2019) Day surgery for anterior cruciate ligament reconstruction in children: a prospective study on feasibility and satisfaction. J Child Orthop 13:100–106
Bareka M, Hantes M, Arnaoutoglou E, Vretzakis G (2018) Superior perioperative analgesia with combined femoral–obturator–sciatic nerve block in comparison with posterior lumbar plexus and sciatic nerve block for ACL reconstructive surgery. Knee Surg Sports Traumatol Arthrosc 26:478–484
Baverel L, Cucurulo T, Lutz C, Colombet CJ, Dalmay F et al (2016) Anesthesia and analgesia methods for outpatient anterior cruciate ligament reconstruction. Orthop Traumatol Surg Res 102:S251–S255
Bromage PR (1965) A comparison of the hydrochloride and carbon dioxide salts of lidocaine and prilocaine in epidural analgesia. Acta Anaesthesiol Scand 9:55–69
Cappelleri G, Casati A, Fanelli G, Borghi B, Anelati D, Berti M (2000) Unilateral spinal anesthesia or combined sciatic-femoral nerve block for day-case knee arthroscopy. A prospective, randomized comparison. Minerva Anestesiol 66:131–136
Davarci I, Tuzcu K, Karcioglu M, Hakimoglu S, Özden R, Yengil E et al (2013) Comparison between ultrasound-guided sciatic-femoral nerve block and unilateral spinal anaesthesia for outpatient knee arthroscopy. J Int Med Res 41:1639–1647
Fanelli G, Casati A, Garancini P, Torri G (1999) Nerve stimulator and multiple injection technique for upper and lower limb blockade. Anesth Analg 88(4):847–852
Gazendam A, Ekhtiari S, Horner NS, Nucci N, Dookie J, Ayeni OR (2021) Perioperative nonopioid analgesia reduces postoperative opioid consumption in knee arthroscopy: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc 29:1887–1903
Goyal T, Das L, Paul S, Choudhury AK, Sethy SS (2021) Outcomes of retro-drilled all-inside tibial tunnel vs complete tibial tunnel techniques in anterior cruciate ligament reconstruction-a comparative study. Eur J Orthop Surg Traumatol. https://doi.org/10.1007/s00590-021-03011-2
Imbelloni LE, de Rezende GVP, Ganem EM, Cordeiro JA (2010) Comparative study between combined sciatic-femoral nerve block, via a single skin injection, and spinal block anesthesia for unilateral surgery of the lower limb. Brazilian J Anesthesiol 60:584–592
Laoruengthana A, Jarusriwanna A, Rattanaprichavej P, Eiamjumras W, Kositanurit I, Pongpirul K (2022) Additional peripheral nerve block to periarticular injection has no benefit for patients undergoing TKA: a factorial propensity score-matched analysis comparing four multimodal analgesic techniques. J Arthroplasty 37:39–44
Maheshwer B, Knapik DM, Polce EM, Verma NN, LaPrade RF, Chahla J (2021) Contribution of multimodal analgesia to postoperative pain outcomes immediately after primary anterior cruciate ligament reconstruction: a systematic review and meta-analysis of level 1 randomized clinical trials. Am J Sports Med 49:3132–3144
Markiewitz ND, Swarup I, Talwar D, Muhly WT, Wells L, Williams BA (2022) Perioperative pain management practices vary across time and setting for pediatric ACL reconstruction: trends from a national database in the United States. Orthop J Sport Med 10(1):23259671211068830
Montes FR, Zarate E, Grueso R, Giraldo JC, Venegas MP, Gomez A (2008) Comparison of spinal anesthesia with combined sciatic-femoral nerve block for outpatient knee arthroscopy. J Clin Anesth 20:415–420
Muench LN, Wolf M, Kia C, Berthold DP, Cote MP, Fischler A et al (2021) A reduced concentration femoral nerve block is effective for perioperative pain control following ACL reconstruction: a retrospective review. Arch Orthop Trauma Surg Arch Orthop Trauma Surg. https://doi.org/10.1007/s00402-021-04221-3
Myles PS, Myles DB, Galagher W, Boyd D, Chew C, MacDonald N et al (2017) Measuring acute postoperative pain using the visual analog scale: the minimal clinically important difference and patient acceptable symptom state. Br J Anaesth 118:424–429
Nakase J, Shimozaki K, Asai K, Yoshimizu R, Kimura M, Tsuchiya H (2021) Usefulness of lateral femoral cutaneous nerve block in combination with femoral nerve block for anterior cruciate ligament reconstruction: a prospective trial. Arch Orthop Trauma Surg 141:455–460
Norman GR, Sloan JA, Wyrwich KW (2003) Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med Care 41:582–592
Sansone V, De Ponti A, Fanelli G, Agostoni M (1999) Combined sciatic and femoral nerve block for knee arthroscopy: 4 years’ experience. Arch Orthop Trauma Surg 119:163–167
Secrist ES, Freedman KB, Ciccotti MG, Mazur DW, Hammoud S (2016) Pain management after outpatient anterior cruciate ligament reconstruction: a systematic review of randomized controlled trials. Am J Sports Med 44:2435–2447
Sehmbi H, Brull R, Shah UJ, El-Boghdadly K, Nguyen D, Joshi GP et al (2019) Evidence basis for regional anesthesia in ambulatory arthroscopic knee surgery and anterior cruciate ligament reconstruction: part II: adductor canal nerve block-a systematic review and meta-analysis. Anesth Analg 128:223–238
Sengoku T, Nakase J, Morita Y, Asai K, Yoshimizu R, Kimura M et al (2022) Anterior cruciate ligament reconstruction with ultrasound-guided femoral nerve block does not adversely affect knee extensor strength beyond that seen with intravenous patient-controlled analgesia at 3 and 6 months postoperatively. Knee 34:252–258
Smith JRH, Belk JW, Kraeutler MJ, Houck DA, Scillia AJ, McCarty EC (2020) Adductor canal versus femoral nerve block after anterior cruciate ligament reconstruction: a systematic review of level I randomized controlled trials comparing early postoperative pain, opioid requirements, and quadriceps strength. Arthroscopy 36(7):1973–1980
Spasiano A, Flore I, Pesamosca A, Della Rocca G (2007) Comparison between spinal anaesthesia and sciatic-femoral block for arthroscopic knee surgery. Minerva Anestesiol 73:13–21
Stebler K, Martin R, Kirkham KR, Lambert J, De Sede A, Albrecht E (2019) Adductor canal block versus local infiltration analgesia for postoperative pain after anterior cruciate ligament reconstruction: a single centre randomised controlled triple-blinded trial. Br J Anaesth 123:e343–e349
Tharwat AI (2011) Combined posterior lumbar plexus-sciatic nerve block versus combined femoral-obturator-sciatic nerve block for ACL reconstruction. Local Reg Anesth 4:1–6
Wassef MR (1993) Interadductor approach to obturator nerve blockade for spastic conditions of adductor thigh muscles. Reg Anesth 18:13–17
Williams BA, Vogt MT, Kentor ML, Figallo CM, Kelly MD, Williams JP (2004) Nausea and vomiting after outpatient ACL reconstruction with regional anesthesia: are lumbar plexus blocks a risk factor? J Clin Anesth 16:276–281
Xue Q, Jiang W, Wang M, Sui J, Wang Y (2020) Femoral nerve block vs adductor canal block after anterior cruciate ligament reconstruction under general anesthesia: a prospective randomized trial protocol. Medicine 99:e20776
Yung EM, Brull R, Albrecht E, Joshi GP, Abdallah FW (2019) Evidence basis for regional anesthesia in ambulatory anterior cruciate ligament reconstruction: part III: local instillation analgesia-a systematic review and meta-analysis. Anesth Analg 128(3):426–437
Zhang L, Tong Y, Li M, Niu X, Zhao X, Lin F (2015) Sciatic-femoral nerve block versus unilateral spinal anesthesia for outpatient knee arthroscopy: a meta-analysis. Minerva Anestesiol 81:1359–1368
Funding
There is no funding source.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The institutional ethics committee approved the study (AIIMS/IEC/17/128).
Availability of data and materials: The data are available on request.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Goyal, T., Paul, S., Choudhury, A.K. et al. Combined femoral–obturator–sciatic nerve block has superior postoperative pain score and earlier ambulation as compared to spinal anaesthesia for arthroscopic anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 30, 3480–3487 (2022). https://doi.org/10.1007/s00167-022-06955-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-022-06955-y