
Abstract
Purpose
The fragility index (FI) is a metric to evaluate the robustness of statistically significant results. It describes the number of patients who would need to change from a non-event to an event to change a result from significant to non-significant. This systematic survey aimed to evaluate the feasibility of applying the FI to findings related to anterior cruciate ligament (ACL) reconstruction in the Scandinavian knee ligament registries.
Methods
The PubMed, EMBASE, Cochrane Library and AMED databases were searched. Studies from the Scandinavian knee ligament registers were eligible if they reported a statistically significant result (p < 0.05) for any of the following dichotomous outcomes; ACL revision, contralateral ACL reconstruction or the presence of postoperative knee laxity. Only studies with a two-arm comparative analysis were included. Eligibility assessment, data extraction and quality assessment were performed by two independent reviewers. The dichotomous analyses were stratified according to the grouping variable for the two comparative arms as follows; age, patient sex, activity at injury, graft choice, drilling technique, graft fixation, single- versus double-bundle, concomitant cartilage injury and country. The two-sided Fisher’s exact test was used to calculate the FI of all statistically significant analyses.
Results
From 158 identified studies, 13 studies were included. They reported statistical significance for a total of 56 dichotomous analyses, of which all but two had been determined by a time-to-event analysis. The median sample size for the arms was 5540 (range 92–38,666). The mean FI for all 56 dichotomous analyses was 80.6 (median 34.5), which means that a mean of 80.6 patients were needed to change outcome status to generate a non-significant result instead of a significant one. Seventeen analyses (30.4%) immediately became non-significant when performing the two-sided Fisher’s exact test and, therefore, had an FI of 0. The analyses related to age were the most robust, with a mean FI of 178.5 (median 116, range 1–1089). The mean FI of the other grouping variables ranged from 0.5 to 48.0.
Conclusion
There was large variability in the FI in analyses from the Scandinavian knee ligament registries and almost one third of the analyses had an FI of zero. The FI is a rough measurement of robustness when applied to registry studies, however, future studies are needed to determine the most appropriate metric for robustness in registry studies. The use of the FI can provide clinicians with a deeper understanding of significant study results and promotes an evidence-based approach in the clinical care of patients.
Level of evidence
Systematic review of prospective cohort studies, Level II.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
A large number of studies related to anterior cruciate ligament (ACL) reconstruction have been published from the Scandinavian knee ligament registries over the past decade [1, 2]. Many of these studies have aimed to determine predictors and risk factors for an additional ACL reconstruction, i.e. a revision or a contralateral ACL reconstruction, or used the presence of postoperative laxity as a measurement of primary ACL reconstruction failure [2]. A P value of less than 0.05 or a 95% confidence interval (CI) excluding the defined null value have been used as the threshold of significance when drawing conclusions on statistically significant predictors. Meeting these criteria implies that the null hypothesis, stating that there would be no difference in outcome depending on the investigated predictor, has been rejected, meaning that the predictor is likely to have a true effect on the outcome after ACL reconstruction.
The concept of a P value was first described by Sir Ronald Fisher and aids in the interpretation of a given result [3]. Although Fisher never did set a threshold for significance, a P value of less than 0.05 shows that a result that is similar to or more extreme than that observed would be found in fewer than 5% of repeated tests, on condition that the null hypothesis was true. It is therefore commonly accepted that a level of significance of 5% is sufficient to conclude that the observed result has not occurred by chance. Nonetheless, the P value says nothing about the robustness of an analysis and the interpretation of P values is many times misunderstood by researchers [4,5,6]. The fragility index (FI) was developed to evaluate the robustness of significant findings in randomised controlled trials (RCTs). More specifically, the FI describes the minimum number of patients in the group with the fewest events that would need to change from a non-event to an event to change the result from significant to non-significant [7]. Although the FI has not previously been applied to registry studies, it should follow the same principle. For example, there are studies from the Scandinavian knee ligament registries reporting that the use of hamstring tendon (HT) autograft significantly increases the risk of ACL revision compared with the use of patellar tendon (PT) autograft [8,9,10]. The FI for these studies would describe how many patients in the PT group would need to change from not undergoing an ACL revision to undergoing one to change the analysis to non-significant. The FI is thus a measurement of the number of events (e.g., ACL revisions) on which the statistical significance depends. In other words; the lower the FI, the more fragile the result.
Recently, the FI was evaluated for 48 RCTs in sports medicine and arthroscopic surgery [11]. Worryingly, the median FI of the included studies was two [11], meaning that drawing conclusions in current clinical trials of sports medicine is in fact based on the outcome of a very limited number of patients. One of the main methodological strengths of the Scandinavian registries is the prospective data collection from a large population. In fact, the registries together comprise data from over 70,000 primary ACL reconstructions [12]. Large study samples increase the robustness of a statistical analysis, however, the FI of the statistically significant findings presented from the Scandinavian registries has not been evaluated. This is important knowledge since it allows for a more precise interpretation of the results and promotes an evidence-based approach in the clinical care of patients. The purpose of this systematic survey was to evaluate the applicability of the FI to registry studies by determining the FI of all analyses from the Scandinavian registries related to any of the following dichotomised outcomes; ACL revision, contralateral ACL reconstruction and the presence of postoperative residual knee laxity.
Materials and methods
Eligibility criteria
Original studies written in English from the Danish, Norwegian and Swedish knee ligament registries were eligible for inclusion if they reported statistically significant results for any of the following dichotomous outcomes; ACL revision, contralateral ACL reconstruction, or the presence of residual knee laxity after ACL reconstruction. A statistically significant result was defined as a P value of < 0.05 or a 95% CI excluding a null value, under the null hypothesis that there would be no difference between groups. For ratio calculations, such as relative risk calculations, odds ratios or hazard ratio calculations, the definition of significance was a 95% CI excluding one. Only studies comparing a dichotomised outcome between two study groups were included, including studies using a dichotomised time-to-event analysis. Studies were excluded if information needed to calculate the FI was missing, e.g., data on the number/proportion of patients in each group, or the number/proportion of events in each group. For studies where only a proportion (%) was presented, the number of patients or the number of events was calculated for each group. Additionally, studies including data from registries outside Scandinavia were excluded.
Literature search
The literature search was performed by an expert in electronic search methods at the Sahlgrenska University Hospital library on 9 May 2017. An updated literature search was performed on 20 April 2018. The searched databases were the PubMed, EMBASE, the Cochrane Library and AMED electronic databases. Search terms were mapped to relevant MeSH terms or subject headings where possible. Three concepts were used to enter search terms into the databases: Concept 1—‘Register’, ‘registry’, ‘registers’, and ‘registries’. Concept 2—‘Sweden’, ‘Swedish’, ‘Denmark’, ‘Danish’, ‘Norway’, ‘Norwegian’, ‘Scandinavia’, ‘Scandinavian’ and ‘Nordic countries’. Concept 3—‘Anterior cruciate ligament’, ‘Anterior cruciate ligament injuries’, ‘Anterior cruciate ligament reconstruction’, ‘Posterior cruciate ligament’ and ‘Posterior cruciate ligament reconstruction’. The ‘OR’ operator was used to group the keywords in each concept. Subsequently, the results from each concept were combined with the ‘AND’ operator. In addition, an e-mail was sent to the registry holder of each Scandinavian registry with a request for a list of publications from the registry. Two authors independently screened all abstracts and full texts, where needed, to identify eligible studies.
Data extraction
Data were extracted independently by two authors using an electronic piloted form (Microsoft Excel, Microsoft Corp; Version 1812). The following data were extracted for each included study; total sample size, specification of the dichotomous outcome measurement, specification of the grouping variable, number of patients in each group, number of patients experiencing an event (the outcome) in each group, the unadjusted and adjusted (where applicable) statistically significant P value or 95% CI and information on the statistical analysis. All statistically significant results from a study originating from a dichotomous analysis by comparing two groups were extracted. So, if a study performed more than one two-group comparison for a dichotomous outcome, data for each analysis were extracted. If there was any disagreement, it was resolved by consulting a third author.
Outcome
The dichotomised outcomes considered for this review were additional ACL reconstruction (either revision or contralateral ACL reconstruction) or postoperative knee joint laxity (yes/no). The dichotomous evaluation of postoperative knee joint laxity was defined according to the definition used in the original studies, i.e. positive pivot shift test (yes/no) and increased anteroposterior laxity of > 2 mm compared with the healthy knee (yes/no).
Quality assessment
A standardised method for assessing internal validity (bias) in registry studies is lacking. The Downs and Black checklist for randomised and non-randomised studies primarily assesses the reporting quality of studies [13] and was determined to be the best available tool for quality assessment in this study. The checklist originally comprised 27 items scored on a 0–2 scale, yielding a maximum score of 30 points. Items number 14, 15, 23 and 24 are related to randomisation and were, therefore, excluded due to not being applicable to the included studies. Similarly, item 27 (power analysis) and item 21 could not be applied to the included studies. Item 21 was excluded as all the studies aiming to analyse two or more registries would score zero (patients not recruited from the same population), even though the quality of the multi-registry studies could be high. Therefore, a modified checklist yielding a maximum score of 22 points was used. Each study was assessed independently by two authors.
Statistical analysis
The FI was calculated using two-by-two tables, according to the method described by Walsh et al. [7]. The P values for the extracted original data were first recalculated by applying a two-sided Fisher’s exact test. If the result was still significant (p < 0.05), the FI was calculated by adding the number of events to the group with the fewest number of events (or lowest risk of event/outcome), while subtracting the same number from the non-events in the group to keep the group sample size constant. Events were added until the P value of the two-sided Fisher’s exact test was no longer significant (p ≥ 0.05). The smallest number of patients that were required to change from a non-event to an event to obtain a p ≥ 0.05 was defined as the FI. All calculations were performed using Microsoft Excel (Microsoft Corp; Version 1812) and SPSS version 25 (IBM Corp; 2017).
The common methodology for reporting the FI for RCTs has been to report only one FI per study, by limiting the FI calculation to only the primary outcome measurement or the first statistically significant result presented in the study abstract [7, 11]. Registry studies often perform multiple analyses for a dichotomous outcome. For example, the dichotomous outcome of ACL revision may be compared between two age groups, two ACL graft choices and two graft fixation devices in the same study. The FI was, therefore, calculated for all the statistically significant results in each study and the results were organised and reported according to the specific predictor studied, i.e., the grouping variable. The grouping variables were classified as either patient- or surgery-related and reported under separate subheadings for readability purposes. Additionally, a subanalysis for the mean and median FI was performed after excluding analyses with an FI of zero. An FI of zero is thought to describe a highly fragile significance, as it means that zero patients need to change from a non-event to an event in order not to obtain significance when applying Fisher’s exact test to the analysis. However, as most studies from the Scandinavian knee ligament registries originally used statistics other than Fisher’s exact test [1, 2], there is a risk that using Fisher’s exact test might underestimate the FI. An FI of zero would be the most extreme underestimation and the subanalysis was therefore performed to compare the overall FI with and without analyses with an FI of zero.
Results
Study selection
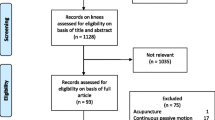
The literature search yielded a total of 157 studies assessed for eligibility and one additional study was identified via communication with a registry holder. After a full-text review, 26 studies originating solely from the Scandinavian registries remained, which also reported on additional ACL reconstruction or postoperative residual knee laxity. Of these, two studies were excluded, as they did not perform any dichotomised statistical test [14, 15], one study was excluded due to not reporting any statistically significant result [16] and three studies were excluded due to applying a statistical analysis that did not enable FI calculation [17,18,19]. The remaining 20 studies reported at least one dichotomous outcome with statistical significance and a statistical test that enabled the calculation of FI. However, seven of these studies were excluded on the basis of not reporting the data needed for the calculation of the FI [20,21,22,23,24,25,26]. Finally, 13 studies were included for further analysis. The study selection process is presented in Fig. 1 and Online Appendix 1 presents the reason for excluding the studies that reported on additional ACL reconstruction or residual knee laxity.

The study selection process. FI fragility index
Overall study characteristics
The 13 included studies had a total of 56 separate dichotomous analyses, of which 49 analyses determined the outcome of ACL revision, three determined the outcome of a contralateral ACL reconstruction, three determined the outcome of residual knee laxity one year postoperatively and one analysis determined the outcome of either an ACL revision or a contralateral ACL reconstruction. The following variables were identified as determining the groups in the studies; age [8, 27,28,29,30,31], patient sex [30], activity at the time of injury [8, 32], HT versus PT autograft [8,9,10], femoral drilling technique [28, 33], graft fixation technique [27, 34, 35], single- versus double-bundle ACL reconstruction [27, 36], concomitant cartilage injury [8, 28, 30] and country where the ACL reconstruction was performed [27]. The Downs and Black score ranged from 13 to 18, with a median score of 17 of a maximum possible score of 22 (Table 1).
The median sample size for the arms was 5540 (range 92–38,666). The median in sample size difference between the two arms was 5464.5 patients (range 26–31,930). The median number of events for the outcome of additional ACL reconstruction (ACL revision or contralateral ACL reconstruction) was 159 (range 9–1171) and for residual laxity 264 (range 195–729). The mean FI for all 56 dichotomous analyses was 80.6, while the median was 34.5. Seventeen analyses (30.4%) became non-significant when performing the two-sided Fisher’s exact test to their contingency table and had therefore an FI of 0. All the analyses are summarised in Tables 2 and 3.
Patient-related factors
The following variables were identified as patient-related; age [8, 27,28,29,30,31], patient sex [30] and activity at time of injury [8, 32]. A total of 19 two-arm analyses for age (18 related to the outcome of ACL revision and one to contralateral ACL reconstruction) were identified. The FI for age ranged from 1 to 1089, with a mean FI of 178.5 and a median of 116.0. The analysis on patient sex as a factor for contralateral ACL reconstruction had an FI of 35.0. There were six analyses on activity at time of injury (five related to the outcome of ACL revision and one to either ACL revision or a contralateral ACL reconstruction). The FI for these analyses ranged from 0 to 53, with a mean FI of 16.0 and a median of 5.5. All analyses with a patient-related factor as the grouping variable are summarised in Table 2.
Surgery-related factors
The following variables were identified as surgery-related; HT versus PT autograft [8,9,10], femoral drilling technique [28, 33], graft fixation [27, 34, 35], single- versus double-bundle ACL reconstruction [27, 36], concomitant cartilage injury [8, 28, 30] and country where the ACL reconstruction was performed [27]. With regard to HT versus PT autograft, three analyses were related to the outcome of ACL revision and one analysis to the outcome of a positive pivot shift one year postoperatively. The FI ranged from 0 to 40, with a mean FI of 15.0 and median of 10.0. The drilling technique comparisons were made between transtibial drilling and the anteromedial or transportal drilling technique (four analyses related to the outcome of ACL revision, one to the outcome of a positive pivot shift test at one year postoperatively and one to the outcome of > 2 mm sagittal laxity at one year postoperatively). The FI ranged from 0 to 159, with a mean FI of 48.0 and a median of 17.0. Graft fixation was investigated in 12 two-arm analyses. The FI ranged from 0 to 216, with a mean FI of 37.4 and a median of 1.0. Single- versus double-bundle was investigated in four analyses, with an FI ranging from 0 to 2 (mean FI 0.5 and median FI 0). With regard to concomitant cartilage injury, there were two analyses related to the outcome of ACL revision and one to contralateral ACL reconstruction. The FI ranged from 0 to 50, with a mean FI of 19.7 and a median of 9.0. With regard to country where the ACL reconstruction was performed, one analysis related to the outcome of ACL revision. The FI of the significant difference between the countries was 130. All analyses with a surgery-related factor as the grouping variable are summarised in Table 3.
Subanalysis
When excluding the 17 analyses with an FI of 0, a total of 39 analyses remained. The FI of those analyses ranged from 1 to 1089, with a mean FI of 115.7 and a median FI of 87.0 (data not shown).
Discussion
This most important finding of this study was that the FI varied substantially across dichotomous analyses from the Scandinavian knee ligament registries. Although almost one third of the analyses had an FI of zero, the analyses related to age generally had the most robust FI, with a mean FI of 178.5 (range 1–1089). In fact, the majority of the analyses had a higher FI than what previously has been reported from RCTs related to orthopaedic surgery [11, 37]. However, the variable FI underlines that there are difficulties in the interpretation of robustness in analyses from these registry studies.
The FI has previously been applied exclusively to RCTs. A median FI of 2 (IQR 1–3) was reported when assessed in 40 RCTs related to orthopaedic spine surgery [37]. Similarly, a median FI of 2 (IQR 1–2.8) was found in 48 RCTs related to arthroscopy and sports medicine surgery [11]. It was concluded that the statistical significance in current orthopaedic RCTs is fragile and that relatively small sample sizes and few outcome events are contributory factors [37]. The large study samples provided by registry studies could theoretically increase the robustness of significant findings. On the other hand, it is not known whether the use of the FI is feasible for registry studies, as there are some fundamental discrepancies in the study design compared with RCTs. A well-designed RCT is thought to exclude confounding factors by assuming an equal distribution of both measured and unmeasured factors due to randomisation and blinding. Registry studies are instead susceptible to confounders and bias, which is commonly dealt with by statistical adjustments. The FI is calculated independently of whether or not the tested P value originates from an adjusted analysis, which is important, as most analyses included in this study were adjusted. Moreover, despite the fact that the FI has previously been applied to time-to-event outcomes in RCTs [7, 11], time-to-event outcomes are more common in registry studies. Time-to-event is not considered when calculating the FI, which means that the FI becomes a rougher measurement for these analyses.
It is obvious that the FI had greater variability in registry studies compared with previous studies of RCTs [11, 37]. The variability of the FI questions the feasibility of using this metric on registry studies, especially since a strong contributor to the variable FI probably is the heterogeneous data analyses. For example, there is no consensus on how to stratify age groups in the Scandinavian knee ligament registry studies. This aggravates a comparison of the FI across studies, since the FI in addition to describe the actual robustness also will be affected by group size and age difference between groups. Moreover, almost one third of the analyses had an FI of zero, which is difficult to interpret for analyses which originally used statistics other than Fisher’s exact test and found significance. Does an FI of zero indicate fragility or is it the result of applying a statistical test that was not deemed to be the most appropriate test in the original study? Interestingly, Walsh et al. [7] applied the FI to 399 trials published in high-impact journals and found that 70% of the trials with an FI of zero originally were analysed using time-to-event analysis [7]. This indicates that time-to-event analyses are particularly susceptible to an FI of zero, which might explain the large proportion of analyses with an FI of zero in this study. Not surprisingly, the mean and median FI were considerably higher when the analyses with an FI of zero were excluded in the subanalysis. Further research is needed to determine the most appropriate methodology for FI calculation in studies using time-to-event analysis. Until then, it could be argued that time-to-event analyses with an FI of zero should be excluded to not severely skew the overall FI.
To draw conclusions regarding the feasibility of using the FI on registry studies, the FI perhaps needs to be assessed in a larger number of registry studies, which could strengthen the data and narrow the range of the FI. That could potentially also enable a determination of the most robust predictors for ACL failure. In this study, most predictors included analyses from only one or two studies. The inclusion of few analyses per predictor makes the FI analysis sensitive to outliers and makes the process of determining the most robust predictor vulnerable. One should however bear in mind that only significant analyses are considered for the FI calculation and few included analyses for a predictor could mean that the reported significance is an exception among several non-significant findings. Patient sex could be used to exemplify this, where only one analysis was included with an FI of 35. Although the FI for patient sex is difficult to interpret based on a single analysis, it should be remembered that seven other studies using ACL revision as the outcome and three other studies using contralateral ACL reconstruction as the outcome found non-significant results when comparing patient sex in the Scandinavian registries [2]. The interpretation of the FI must therefore also be set in the context of the cumulative evidence.
Not all predictors were, however, limited by few analyses, and the feasibility of using the FI is strengthened when determining the FI for the two predictors with most analyses (age with 19 analyses and graft fixation with 12 analyses), as the result reflects previous literature on the subject. The literature is unanimous when it comes to young age as a risk factor for an additional ACL reconstruction [38,39,40,41,42]. In agreement with this, the FI for age was by far the highest, which indicates that the FI calculation is able to provide a reliable estimate of robustness. This is further emphasised by the higher FI in analyses with an increasing age difference between the compared groups. With regard to graft fixation, six of 12 analyses had an FI of 0 and the mean FI for all the analyses was 37.4. For this reason, graft fixation does not predict an additional ACL reconstruction with the same certainty as age, which is supported by the contradictory literature regarding the impact of graft fixation [43,44,45].
In the light of the limitations associated with using the FI on registry studies, it is our opinion that the FI could be regarded as a rough measurement of robustness for registry studies and that it could be used to compare confidence in the results across analyses with a similar statistical methodology. There is reason to believe that the FI could be a valuable method for registry studies, especially for those using statistical methods that are perfectly compatible with the FI, such as Chi-square or Fisher’s exact test. The large amount of data comprised in registries should intuitively increase the robustness, but it is important to find a metric to quantify this objectively in registry studies. Although there might be outcomes in registry studies that are more or less appropriate for the use of FI, researchers should be encouraged to calculate and report the FI whenever possible. The strength in numbers of registry studies does not compensate for other limitations, such as confounders, bias and an inability to provide causality. Care must be taken not to overestimate the effect of a higher FI in registry studies compared with RCTs, as RCTs still remain the gold standard to determine the efficacy of an intervention. This study is also limited by the fact that analyses from seven studies needed to be excluded, as data on study arm size and the number of events were not reported. Future studies should preferably report these numbers. It should also be mentioned that the outcome of additional ACL reconstruction may underestimate the true rate of failed ACL reconstructions. This becomes especially relevant to consider in studies with small FIs, since the robustness of significance in these circumstances is likely to be even more vulnerable to “hidden” failures not proceeding to an ACL revision.
Conclusion
There was large variability in the FI in analyses from the Scandinavian knee ligament registries and almost one third of the analyses had an FI of zero. The FI is a rough measurement of robustness when applied to registry studies, however, future studies are needed to determine the most appropriate metric for robustness in registry studies. The use of the FI can provide clinicians with a deeper understanding of significant study results and promotes an evidence-based approach in the clinical care of patients.
References
Hamrin Senorski E, Svantesson E, Baldari A, Ayeni OR, Engebretsen L et al (2019) Factors that affect patient reported outcome after anterior cruciate ligament reconstruction—a systematic review of the Scandinavian knee ligament registers. Br J Sports Med 53(7):410–417
Svantesson E, Hamrin Senorski E, Baldari A, Ayeni OR, Engebretsen L et al (2019) Factors associated with additional anterior cruciate ligament reconstruction and register comparison: a systematic review on the Scandinavian knee ligament registers. Br J Sports Med 53(7):418–425
Fisher R (1973) Statistical methods and scientific inference, 3rd edn. Hafner Publishing Company, New York
Cohen HW (2011) P values: use and misuse in medical literature. Am J Hypertens 24(1):18–23
Kyriacou DN (2016) The enduring evolution of the p value. JAMA 315(11):1113–1115
Mark DB, Lee KL, Harrell FE Jr (2016) Understanding the role of p values and hypothesis tests in clinical research. JAMA Cardiol 1(9):1048–1054
Walsh M, Srinathan SK, McAuley DF, Mrkobrada M, Levine O et al (2014) The statistical significance of randomized controlled trial results is frequently fragile: a case for a fragility index. J Clin Epidemiol 67(6):622–628
Gifstad T, Foss OA, Engebretsen L, Lind M, Forssblad M et al (2014) Lower risk of revision with patellar tendon autografts compared with hamstring autografts: a registry study based on 45,998 primary ACL reconstructions in Scandinavia. Am J Sports Med 42(10):2319–2328
Persson A, Fjeldsgaard K, Gjertsen JE, Kjellsen AB, Engebretsen L et al (2014) Increased risk of revision with hamstring tendon grafts compared with patellar tendon grafts after anterior cruciate ligament reconstruction: a study of 12,643 patients from the Norwegian cruciate ligament registry, 2004–2012. Am J Sports Med 42(2):285–291
Rahr-Wagner L, Thillemann TM, Pedersen AB, Lind M (2014) Comparison of hamstring tendon and patellar tendon grafts in anterior cruciate ligament reconstruction in a nationwide population-based cohort study: results from the Danish registry of knee ligament reconstruction. Am J Sports Med 42(2):278–284
Khan M, Evaniew N, Gichuru M, Habib A, Ayeni OR et al (2017) The fragility of statistically significant findings from randomized trials in sports surgery: a systematic survey. Am J Sports Med 45(9):2164–2170
Prentice HA, Lind M, Mouton C, Persson A, Magnusson H et al (2018) Patient demographic and surgical characteristics in anterior cruciate ligament reconstruction: a description of registries from six countries. Br J Sports Med 52(11):716–722
Downs SH, Black N (1998) The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Commun Health 52(6):377–384
Lind M, Menhert F, Pedersen AB (2009) The first results from the Danish ACL reconstruction registry: epidemiologic and 2 year follow-up results from 5818 knee ligament reconstructions. Knee Surg Sports Traumatol Arthrosc 17(2):117–124
Rahr-Wagner L, Thillemann TM, Lind MC, Pedersen AB (2013) Validation of 14,500 operated knees registered in the Danish knee ligament reconstruction register: registration completeness and validity of key variables. Clin Epidemiol 5:219–228
Bjornsson H, Andernord D, Desai N, Norrby O, Forssblad M et al (2015) No difference in revision rates between single- and double-bundle anterior cruciate ligament reconstruction: a comparative study of 16,791 patients from the Swedish national knee ligament register. Arthroscopy 31(4):659–664
Andernord D, Desai N, Bjornsson H, Ylander M, Karlsson J et al (2015) Patient predictors of early revision surgery after anterior cruciate ligament reconstruction: a cohort study of 16,930 patients with 2-year follow-up. Am J Sports Med 43(1):121–127
Eysturoy NH, Nissen KA, Nielsen T, Lind M (2018) The influence of graft fixation methods on revision rates after primary anterior cruciate ligament reconstruction. Am J Sports Med 46(3):524–530
Snaebjornsson T, Hamrin Senorski E, Ayeni OR, Alentorn-Geli E, Krupic F et al (2017) Graft diameter as a predictor for revision anterior cruciate ligament reconstruction and KOOS and EQ-5D values: a cohort study from the Swedish national knee ligament register based on 2240 patients. Am J Sports Med 45(9):2092–2097
Andernord D, Bjornsson H, Petzold M, Eriksson BI, Forssblad M et al (2014) Surgical predictors of early revision surgery after anterior cruciate ligament reconstruction: results from the Swedish national knee ligament register on 13,102 patients. Am J Sports Med 42(7):1574–1582
Andernord D, Desai N, Bjornsson H, Gillen S, Karlsson J et al (2015) Predictors of contralateral anterior cruciate ligament reconstruction: a cohort study of 9061 patients with 5-year follow-up. Am J Sports Med 43(2):295–302
Faltstrom A, Hagglund M, Magnusson H, Forssblad M, Kvist J (2016) Predictors for additional anterior cruciate ligament reconstruction: data from the Swedish national ACL register. Knee Surg Sports Traumatol Arthrosc 24(3):885–894
Granan LP, Baste V, Engebretsen L, Inacio MC (2015) Associations between inadequate knee function detected by KOOS and prospective graft failure in an anterior cruciate ligament-reconstructed knee. Knee Surg Sports Traumatol Arthrosc 23(4):1135–1140
Kvist J, Kartus J, Karlsson J, Forssblad M (2014) Results from the Swedish national anterior cruciate ligament register. Arthroscopy 30(7):803–810
Lind M, Menhert F, Pedersen AB (2012) Incidence and outcome after revision anterior cruciate ligament reconstruction: results from the Danish registry for knee ligament reconstructions. Am J Sports Med 40(7):1551–1557
Rahr-Wagner L, Thillemann TM, Lind M, Pedersen AB (2015) Comorbidities in patients with anterior cruciate ligament reconstruction compared with matched controls without anterior cruciate ligament injury from danish registries. Arthroscopy 31(9):1741–1747 (e1744)
Aga C, Kartus JT, Lind M, Lygre SHL, Granan LP et al (2017) Risk of revision was not reduced by a double-bundle ACL reconstruction technique: results from the Scandinavian registers. Clin Orthop Relat Res 475(10):2503–2512
Desai N, Andernord D, Sundemo D, Alentorn-Geli E, Musahl V et al (2017) Revision surgery in anterior cruciate ligament reconstruction: a cohort study of 17,682 patients from the Swedish national knee ligament register. Knee Surg Sports Traumatol Arthrosc 25(5):1542–1554
Fauno P, Rahr-Wagner L, Lind M (2014) Risk for revision after anterior cruciate ligament reconstruction is higher among adolescents: results from the danish registry of knee ligament reconstruction. Orthop J Sports Med 2(10):2325967114552405
Snaebjornsson T, Hamrin Senorski E, Sundemo D, Svantesson E, Westin O et al (2017) Adolescents and female patients are at increased risk for contralateral anterior cruciate ligament reconstruction: a cohort study from the Swedish national knee ligament register based on 17,682 patients. Knee Surg Sports Traumatol Arthrosc 25(12):3938–3944
Soreide E, Granan LP, Hjorthaug GA, Espehaug B, Dimmen S et al (2016) The effect of limited perioperative nonsteroidal anti-inflammatory drugs on patients undergoing anterior cruciate ligament reconstruction. Am J Sports Med 44(12):3111–3118
Ahlden M, Samuelsson K, Sernert N, Forssblad M, Karlsson J et al (2012) The Swedish national anterior cruciate ligament register: a report on baseline variables and outcomes of surgery for almost 18,000 patients. Am J Sports Med 40(10):2230–2235
Rahr-Wagner L, Thillemann TM, Pedersen AB, Lind MC (2013) Increased risk of revision after anteromedial compared with transtibial drilling of the femoral tunnel during primary anterior cruciate ligament reconstruction: results from the Danish knee ligament reconstruction register. Arthroscopy 29(1):98–105
Persson A, Gifstad T, Lind M, Engebretsen L, Fjeldsgaard K et al (2018) Graft fixation influences revision risk after ACL reconstruction with hamstring tendon autografts. Acta Orthop 89(2):204–210
Persson A, Kjellsen AB, Fjeldsgaard K, Engebretsen L, Espehaug B et al (2015) Registry data highlight increased revision rates for endobutton/biosure HA in ACL reconstruction with hamstring tendon autograft: a nationwide cohort study from the Norwegian knee ligament registry, 2004–2013. Am J Sports Med 43(9):2182–2188
Svantesson E, Sundemo D, Hamrin Senorski E, Alentorn-Geli E, Musahl V et al (2017) Double-bundle anterior cruciate ligament reconstruction is superior to single-bundle reconstruction in terms of revision frequency: a study of 22,460 patients from the Swedish national knee ligament register. Knee Surg Sports Traumatol Arthrosc 25(12):3884–3891
Evaniew N, Files C, Smith C, Bhandari M, Ghert M et al (2015) The fragility of statistically significant findings from randomized trials in spine surgery: a systematic survey. Spine J 15(10):2188–2197
Kaeding CC, Pedroza AD, Reinke EK, Huston LJ, Spindler KP (2015) Risk factors and predictors of subsequent ACL injury in either knee after ACL reconstruction: prospective analysis of 2488 primary ACL reconstructions from the MOON Cohort. Am J Sports Med 43(7):1583–1590
Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE (2014) Incidence of second ACL injuries 2 years after primary ACL reconstruction and return to sport. Am J Sports Med 42(7):1567–1573
Webster KE, Feller JA (2016) Exploring the high reinjury rate in younger patients undergoing anterior cruciate ligament reconstruction. Am J Sports Med 44(11):2827–2832
Webster KE, Feller JA, Leigh WB, Richmond AK (2014) Younger patients are at increased risk for graft rupture and contralateral injury after anterior cruciate ligament reconstruction. Am J Sports Med 42(3):641–647
Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE et al (2016) Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med 44(7):1861–1876
Browning WM 3rd, Kluczynski MA, Curatolo C, Marzo JM (2017) Suspensory versus aperture fixation of a quadrupled hamstring tendon autograft in anterior cruciate ligament reconstruction: a meta-analysis. Am J Sports Med 45(10):2418–2427
Hurley ET, Gianakos AL, Anil U, Strauss EJ, Gonzalez-Lomas G (2019) No difference in outcomes between femoral fixation methods with hamstring autograft in anterior cruciate ligament reconstruction—a network meta-analysis. Knee 26(2):292–301
Jiang H, Ma G, Li Q, Hu Y, Li J et al (2018) Cortical button versus cross-pin femoral fixation for hamstring anterior cruciate ligament reconstruction: a meta-analysis of randomized controlled trials. Am J Sports Med 46(9):2277–2284
Funding
This study received no financial support or grant.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Dr. Olufemi R. Ayeni is an educational consultant for the speaker’s bureau of Conmed and Smith & Nephew.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study informed consent was not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Svantesson, E., Hamrin Senorski, E., Danielsson, A. et al. Strength in numbers? The fragility index of studies from the Scandinavian knee ligament registries. Knee Surg Sports Traumatol Arthrosc 28, 339–352 (2020). https://doi.org/10.1007/s00167-019-05551-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05551-x