
Abstract
Purpose
Tranesophageal echocardiography or direct sampling of arterial and/or right atrial blood with histological evaluation are invasive techniques used to evaluate embolic material entering the heart during total knee arthroplasty (TKA). The aim of this study was to develop a non-invasive method of detecting and quantifying the embolic matter using transthoracic echocardiography and to apply this method to compare the incidence and severity of embolism between computer-navigated (N) and conventional (C) TKA done under tourniquet.
Methods
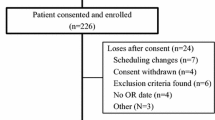
Twenty-eight patients (15 N-TKA and 13 C-TKA) were enrolled. Transthoracic echocardiography was performed in all standard views prior to surgery and continuously after the tourniquet release for monitoring the echodense particulates appearing in the right atrium. To estimate the severity of echogenic embolization, maximum absolute increase in luminosity after tourniquet release (peak embolic load) and area under the curve (AUC; total embolic load) were both calculated.
Results
Twenty-four (85%) had significant particulate matter in right atrium (median time from release of thigh tourniquet to peak embolization in right atrium: 18.0 s). Peak embolic load was lower in N-TKA than C-TKA [17.0 versus 35.0 arbitrary luminosity units, p = 0.03]. Total embolic load, by area under the curve, was lower in the N-TKA group.
Conclusions
Perioperative particulate embolization during TKA can be quantified non-invasively with the use of transthoracic echocardiography and off-line image analysis. N-TKA, by virtue of avoiding intramedullary guides, causes lesser total embolic load and hence can lead to decreased the severity and incidence of this potentially fatal phenomenon.
Level of evidence
II.



Similar content being viewed by others


References
Berman AT, Parmet JL, Harding SP, Israelite CL, Chandrasekaran K, Horrow JC, Singer R, Rosenberg H (1998) Emboli observed with use of transesophageal echocardiography immediately after tourniquet release during total knee arthroplasty with cement. J Bone Jt Surg Am 80:389–396
Bulger EM, Smith DG, Maier RV, Jurkovich GJ (1997) Fat embolism syndrome. A 10-year review. Arch Surg 132:435–439
Caillouette JT, Anzel SH (1990) Fat embolism syndrome following the intramedullary alignment guide in total knee arthroplasty. Clin Orthop Relat Res 251:198–199
Church JS, Scadden JE, Gupta RR, Cokis C, Williams KA, Janes GC (2007) Embolic phenomena during computer-assisted and conventional total knee replacement. J Bone Joint Surg Br 89:481–485
Dorr LD, Merkel C, Mellman MF, Klein I (1989) Fat emboli in bilateral total knee arthroplasty. Predictive factors for neurologic manifestations. Clin Orthop Relat Res 248:112–118
Haytmanek CT, Pour AE, Restrepo C, Nikhil J, Parvizi J, Hozack WJ (2010) Cognition following computer-assisted total knee arthroplasty: a prospective cohort study. J Bone Jt Surg Am 92:92–97
Fahmy NR, Chandler HP, Danylchuk K, Matta EB, Sunder N, Siliski JM (1990) Blood-gas and circulatory changes during total knee replacement. Role of the intramedullary alignment rod. J Bone Jt Surg Am 72:19–26
Johnson MJ, Lucas GL (1996) Fat embolism syndrome. Orthopedics 19:41–48
Kalairajah Y, Cossey AJ, Verrall GM, Ludbrook G, Spriggins AJ (2006) Are systemic emboli reduced in computer-assisted knee surgery?: A prospective, randomised, clinical trial. J Bone Jt Surg Br 88:198–202
Kim YH (2001) Incidence of fat embolism syndrome after cemented or cementless bilateral simultaneous and unilateral total knee arthroplasty. J Arthroplasty 16:730–739
Kim YH, Kim JS, Hong KS, Kim YJ, Kim JH (2008) Prevalence of fat embolism after total knee arthroplasty performed with or without computer navigation. J Bone Jt Surg Am 90:123–128
Kolettis GT, Wixson RL, Peruzzi WT, Blake MJ, Wardell S, Stulberg SD (1994) Safety of 1-stage bilateral total knee arthroplasty. Clin Orthop Relat Res 309:102–109
Lee SC, Yoon JY, Nam CH, Kim TK, Jung KA, Lee DW (2011) Cerebral fat embolism syndrome after simultaneous bilateral total knee arthroplasty a case series. J Arthroplasty. doi:10.1016/j.arth.2011.06.013
Moore P, James O, Saltos N (1981) Fat embolism syndrome: incidence, significance and early features. Aust N Z J Surg 51:546–551
O’Connor MI, Brodersen MP, Feinglass NG, Leone BJ, Crook JE, Switzer BE (2010) Fat emboli in total knee arthroplasty: a prospective randomized study of computer-assisted navigation vs standard surgical technique. J Arthroplasty 25:1034–1040
Ries MD, Rauscher LA, Hoskins S, Lott D, Richman JA, Lynch F Jr (1998) Intramedullary pressure and pulmonary function during total knee arthroplasty. Clin Orthop Relat Res 356:154–160
Smith PN, Leditschke A, McMahon D, Sample RR, Perriman D, Prins A, Brüssel T, Li RW (2008) Monitoring and controlling intramedullary pressure increase in long bone instrumentation: a study on sheep. J Orthop Res 26:1327–1333
ten Duis HJ (1997) The fat embolism syndrome. Injury 28:77–85
Van Gorp CC, Falk JV, Kmiec SJ Jr, Siston RA (2009) The reamer/irrigator/aspirator reduces femoral canal pressure in simulated TKA. Clin Orthop Relat Res 467:805–809
Zanasi S (2011) Innovations in total knee replacement: new trends in operative treatment and changes in peri-operative management. Eur Orthop Traumatol 2:21–31
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Walker, P., Bali, K., Van der Wall, H. et al. Evaluation of echogenic emboli during total knee arthroplasty using transthoracic echocardiography. Knee Surg Sports Traumatol Arthrosc 20, 2480–2486 (2012). https://doi.org/10.1007/s00167-012-1927-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-012-1927-4