
Abstract
Objective: Acute hypoxemic respiratory failure (AHRF) is a common reason for emergency pediatric intensive care. An objective assessment of disease severity from acute physiological parameters would be of value in clinical practice and in the design of clinical trials. We hypothesised that there was a difference in the best early respiratory indices in those who died compared with those who survived.
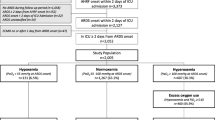
Design: A prospective observational study of 118 consecutive AHRF admissions with data analysis incorporating all blood gases.
Setting: A pediatric intensive care unit in a national children’s hospital.
Interventions: None.
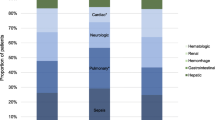
Results: Mortality was 26/118,22% (95% confidence interval 18–26%). There were no significant differences in the best alveolar-arterial oxygen tension gradient (A-aDO2, torr), oxygenation index (OI), ventilation index (VI), or PaO2/FIO2 during the first 2 days of intensive care between the survivors and non-survivors. Only the mean airway pressure (MAP, cm H2O) used for supportive care was significantly different on days 0 and 1 (p≤0.05) with higher pressure being used in non-survivors. Multiple logistic regression analysis did not identify any gas exchange or ventilator parameter independently associated with mortality. Rather, all deaths were associated with coincident pathology or multi-organ system failure, or perceived treatment futility due to pre-existing diagnoses instead of unsupportable respiratory failure. When using previously published predictors of outcome (VI>40 and OI>40; A-aDO2>450 for 24 h; A-aDO2>470 or MAP>23; or A-aDO2>420) the risk of mortality was overestimated significantly in the current population.
Conclusion: The original hypothesis was refuted. It appears that the outcome of AHRF in present day pediatric critical care is principally related to the severity of associated pathology and now no longer solely to the severity of respiratory failure. Further studies in larger series are needed to confirm these findings.
Article PDF
Similar content being viewed by others

References
Lyrene RK, Truog WE (1981) Adult respiratory distress syndrome in a pediatric intensive care unit: predisposing conditions, clinical course and outcome. Pediatrics 67: 790–795
Rivera RA, Butt W, Shann F (1990) Predictors of mortality in children with respiratory failure; possible indications for ECMO. Anaesth Intensive Care 18: 385–389
Tamburro RF, Bugnitz MC, Stidham GL (1991) Alveolar-arterial oxygen gradient as a predictor of outcome in patients with non-neonatal respiratory failure. J Pediatr 119: 935–938
Timmons OD, Dean M, Vernon DD (1991) Mortality rates and prognostic variables in children with adult respiratory distress syndrome. J Pediatr 119: 896–899
Davis SL, Furman DP, Costarino AT (1993) Adult respiratory distress syndrome in children: associated diseases, clinical course and predictors of death. J Pediatr 123: 35–45
Timmons OD, Havens PL, Fackler JC and the Pediatric Critical Care Study Group and the Extracorporeal Life Support Organisation (1995) Predicting death in pediatric patients with acute respiratory failure. Chest 108: 789–797
Hammer J, Numa A, Newth CJL (1997) Acute respiratory distress syndrome caused by respiratory syncytial virus. Pediatr Pulmonol 23: 176–183
Goldman AP, Tasker RC, Hosiasson S, Henrichsen T, Macrae DJ (1997) Early response to inhaled nitric oxide and its relationship to outcome in children with severe hypoxemic respiratory failure. Chest 112: 752–758
Sarnaik AP, Meert KL, Pappas MD, Simpson PM, Lieh-Lai MW, Heider-mann SM (1996) Predicting outcome in children with severe acute respiratory failure treated with high-frequency ventilation. Crit Care Med 24: 1396–1402
Bernard GR, Artigas A, Brigham KL, et al. (1994) The American-European consensus conference on ARDS: Definitions, mechanisms, relevant outcomes and clinical trial coordination. Am J Respir Crit Care Med 149: 818–824
Wilkinson JD, Pollock MM, Ruttiman UE, Glass NL, Yeh TS (1986) Outcome of pediatric patients with multiple organ system failure. Crit Care Med 14: 271–274
Jimenez P, Torres A, Roca J, Cobos A, Rodriquez-Roisin R (1994) Arterial oxygenation does not predict the outcome of patients with acute respiratory failure needing mechanical ventilation. Eur Respir J 7: 730–735
Ferring M, Vincent J-L (1997) Is outcome from ARDS related to the severity of respiratory failure? Eur Respir J 10: 1297–1300
Vincent J-L (1994) Outcome from mechanical ventilation. Eur Respir J 7: 640–642
Pollack MM, Patel KM, Ruttimann UE (1996) PRISM III: An updated pediatric risk of mortality score. Crit Care Med 24: 743–752
Shann F, Pearson G, Slater A, Wilkinson K (1997) Paediatric index of mortality (PIM): a mortality prediction model for children in intensive care. Intensive Care Med 23: 201–207
Rowan KM, Kerr JH, Major F, McPher-son K, Short A, Vessey MP (1993) Intensive Care Society’s APACHE II study in Britain and Ireland — I: Variations in case mix of adult admissions to general intensive care units and impact on outcome. BMJ 307: 972–977
Petros AJ, Marshall JC, Van Saene HKF (1995) Should morbidity replace mortality as an end point for clinical trials in intensive care? Lancet 345: 369–371
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Peters, M.J., Tasker, R.C., Kiff, K.M. et al. Acute hypoxemic respiratory failure in children: case mix and the utility of respiratory severity indices. Intensive Care Med 24, 699–705 (1998). https://doi.org/10.1007/s001340050647
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s001340050647