
Abstract
Objective: To investigate adrenocortical function in patients with ruptured aneurysm of the abdominal aorta.
Design: Prospective clinical investigation.
Setting: Surgical intensive care unit in a university teaching hospital and intensive care unit in a general hospital.
Patients and participants: 54 patient with a documented rupture of the abdominal aorta.
Interventions: A short adrenocorti-cotrophic hormone (ACTH) stimulation test was performed.
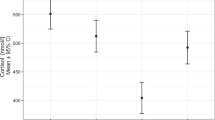
Measurements and results: Patients were studied within 24 h of admission to the hospital. Blood samples for the measurement of cortisol and ACTH were collected at 0800 h. Subsequently 0.25 mg tetracosactrin (Synacthen) was injected i. v. and after 60 min cortisol measurement was repeated. The criterion for a normal short ACTH test was: stimulated or unstimulated cortisol levels ≥ 0.55 µmol/1. For the group as a whole, an unstimulated plasma cortisol level of 0.76 µmol/l was comparable to that in other groups of critically ill patients with similar severity of illness. Between survivors and non survivors, significant differences were found between unstimulated plasma cortisol levels (0.70 vs 1.03 µmol/l), stimulated plasma cortisol levels (1.00 vs 1.30 µmol/1), and plasma ACTH levels (72 vs 133 ng/1). One patient did not meet the criteria for normal adrenocortical function: unstimulated plasma cortisol 0.26 µmol/1, stimulated plasma cortisol 0.47 µmol/1.
Conclusions: In the patients studied with ruptured aneurysm of the abdominal aorta, adrenocortical response was comparable to that in other groups of critically ill patients with similar severity of illness. High cortisol levels were associated with mortality. One patient did not meet the criteria for normal adrenocortical function but survived without steroid treatment.
Similar content being viewed by others


References
Case Records of the Massachusets General Hospital (1985) N Engl J Med 312:976–983
Dorin RI, Kearns PJ (1988) High output circulatory failure in acute adrenal insufficiency. Crit Care Med 16: 296–297
Gleadle J, Varma N, Raggatt PR, Park GR (1991) Adrenal insufficiency in critically ill patients. Clin Intensive Care 2:104–105
Tromp Meesters RC, van der Graaf Y, Vos A, Eikelboom BC (1994) Ruptured aneurysm: early postoperative prediction of mortality using an organ system failure score. British Journal of Surgery 81: 512–516
Roumen RMH, Hendriks T, van der Veen-Jongekrijg J, Nieuwenhuizen GAP, Sauerwein RW, van der Meer JWM, Goris RJA (1993) Cytokine patterns in patients after major vascular surgery, hemorrhagic shock and severe blunt trauma: relation with subsequent ARDS and MOF. Ann Surg 218: 769–776
Sori AJ, Rush BF, Lysz TW, Smith SM, Maciedo GW (1988) The gut as source of sepsis after hemorrhagic shock. Am J Surg 155:187–192
May ME, Carey RM (1985) Rapid adrenocorticotropic hormone test in practice. Retrospective review. Am J Med 79: 679–684
Span LFR, Hermus ARMM, Bartelink AKM, Hoitsma AJ, Gimbrere JSF, Smals AGH, Kloppenborg PWC (1992) Adrenocortical function: an indicator of severity of disease and survival in chronic critically ill patients. Intensive Care Med 18: 93–96
Jurney TH, Cockrell JL, Lindberg JS, Lamiell JM, Wade CE (1987) Spectrum of serum cortisol response to ACTH in ICU patients. Chest 92: 292–295
Rothwell PM, Udwadia ZF, Lawler PG (1991) Cortisol response to corticotro-pin and survival in septic shock. Lancet 337:582–583
Chernow B, Alexander HR, Smallridge RC, Raleigh Thompson W, Cook D, Beardsley D, Fink MP, Lake CR, Fletcher JR (1987) Hormonal responses to graded surgical stress. Arch Intern Med 147:1273–1278
Drucker D, Shandling M (1985) Variable adrenocortical function in acute medical illness. Crit Care Med 13: 477–479
Wade CE, Lindberg JS, Cockrell JL, Lamiell JM, Hunt MM, Ducey J, Jurney TH (1988) Upon-admission adrenal steroidgenesis is adapted to the degree of illness in intensive care unit patients. J Clin Endocrinol Metab 67: 223–227
Vermes I, Beisenhuizen A, Hampsink RM, Haanen C (1995) Dissociation of plasma adrenocorticotropin and cortisol levels in critically ill patients: possible role of endothelin and atrial natriuretic hormone. J Clin Endocrinol Metab 80:1238–1242
Naito Y, Fukata J, Tamai S, Seo N, Nakai Y, Mori K, Imura H (1991) Biphasic changes in hypothalamo-pituitary-adrenal function during the early recovery period after major abdominal surgery. J Clin Endocrinol Metab 73:111–117
Fragen RJ, Shanks CA, Molteni A, Avram MJ (1984) Effects of etomidate on hormonal response to surgical stress. Anesthesiology 61: 652–656
Briegel J, Schelling G, Haller M, Mraz W, Forst H, Peter K (1996) A comparison of the adrenocortical response during septic shock and after complete recovery. Intensive Care Med 22: 894–899
Wagner RL, White PF, Kan PB, Rosenthal MH, Feldman D (1984) Inhibition of adrenal steroidgenesis by the anesthetic etomidate. N Engl J Med 310:1415–1421
McGrady EM, Wright IH (1989) Cardiovascular instability following bolus dose of etomidate. Anaesthesia 44:404–405
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Braams, R., Koppeschaar, H.P.F., van de Pavoordt, H.D.W.M. et al. Adrenocortical function in patients with ruptured aneurysm of the abdominal aorta. Intensive Care Med 24, 124–127 (1998). https://doi.org/10.1007/s001340050532
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s001340050532