
Abstract
Purpose
IntelliVent-ASV® is a development of adaptive support ventilation (ASV) that automatically adjusts ventilation and oxygenation parameters. This study assessed the safety and efficacy of IntelliVent-ASV® in sedated intensive care unit (ICU) patients with acute respiratory failure.
Methods
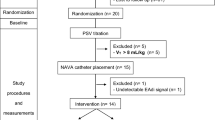
This prospective randomized crossover comparative study was conducted in a 12-bed ICU in a general hospital. Two periods of 2 h of ventilation in randomly applied ASV or IntelliVent-ASV® were compared in 50 sedated, passively ventilated patients. Tidal volume (V T), respiratory rate (RR), inspiratory pressure (P INSP), SpO2 and ETCO2 were continuously monitored and recorded breath by breath. Mean values over the 2-h period were calculated. Respiratory mechanics, plateau pressure (P PLAT) and blood gas exchanges were measured at the end of each period.
Results
There was no safety issue requiring premature interruption of IntelliVent-ASV®. Minute ventilation (MV) and V T decreased from 7.6 (6.5–9.5) to 6.8 (6.0–8.0) L/min (p < 0.001) and from 8.3 (7.8–9.0) to 8.1 (7.7–8.6) mL/kg PBW (p = 0.003) during IntelliVent-ASV® as compared to ASV. P PLAT and FiO2 decreased from 24 (20–29) to 20 (19–25) cmH2O (p = 0.005) and from 40 (30–50) to 30 (30–39) % (p < 0.001) during IntelliVent-ASV® as compared to ASV. RR, P INSP, and PEEP decreased as well during IntelliVent-ASV® as compared to ASV. Respiratory mechanics, pH, PaO2 and PaO2/FiO2 ratio were not different but PaCO2 was slightly higher during IntelliVent-ASV® as compared to ASV.
Conclusions
In passive patients with acute respiratory failure, IntelliVent-ASV® was safe and able to ventilate patients with less pressure, volume and FiO2 while producing the same results in terms of oxygenation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Closed-loop control ventilation refers to the use of a feedback signal (a measured value) to adjust the ventilator outputs in order to meet individual patient’s needs [1]. The commercially available closed-loop ventilation modalities up to now have focused on the support of respiratory muscles [2]. Among them, adaptive support ventilation (ASV) adapts ventilator support in passive patients, transitions patients from controlled to supported modes and automates the weaning process. By adjusting ventilator settings to respiratory mechanics, ASV can select individualized breath patterns [3] with reduced tidal volume (V T) for patients with acute respiratory distress syndrome (ARDS) [4], and reduce weaning duration in post cardiac surgery patients [5] and in ICU patients [6, 7]. IntelliVent-ASV® (Hamilton Medical, Rhäzüns, Switzerland) is a recently released development of ASV that automatically adjusts both ventilation and oxygenation parameters. In short, minute volume is adjusted according to end tidal CO2 (ETCO2) information in passive breathing patients and oxygenation is adjusted according to SpO2 information. This prospective randomized crossover study compared the safety and efficacy of IntelliVent-ASV® with ASV in sedated ICU patients with moderately severe acute respiratory failure.
Patients and methods
The study was conducted from July to December 2009 in the 12-bed medical-surgical adult ICU of Font Pré Hospital in Toulon (France). The regional institutional review board (Comité de Protection des Personnes (CPP) of Nice, France) approved the protocol and signed informed consent was obtained from each patient’s next of kin. The study was registered on ClinicalTrials.gov as NCT01489085.
Patients
Because this study is the first clinical experience of IntelliVent-ASV® in ICU patients, the objective was to include passive stable patients with moderate severity acute respiratory failure. Patients were included if they were invasively and passively ventilated with a sedation Ramsay score of 5 or 6. Exclusion criteria were increased intracranial pressure, severe ARDS requiring a permissive hypercapnia strategy, chronic respiratory failure receiving long-term oxygen therapy and/or home non-invasive ventilation, severe cardiac arrhythmia, therapeutic hypothermia, brain-dead patients, pregnancy and bronchopleural fistula. Patients were orally intubated and mechanically ventilated using an S1 ventilator (Hamilton Medical, Rhäzüns, Switzerland) with IntelliVent-ASV® software (v1.28). At inclusion, patients were ventilated in adaptive support ventilation (ASV) mode as a routine mode of ventilation in the unit [3]. Settings [minute ventilation (MV) and maximum inspiratory pressure] were adjusted to keep tidal volume (V T) below 10 mL/kg of predicted body weight (PBW) with a plateau pressure (P PLAT) below 30 cmH2O. ASV and IntelliVent-ASV® are pressure-limited modes and the maximum inspiratory pressure was kept at 40 cmH2O throughout the study. Patients were kept in a supine position with the head elevated at 45°. For sedation a midazolam–fentanyl combination was used to reach a Ramsay score of 5 or 6 with no spontaneous breathing activity, which was confirmed by the absence of patient’s breath triggering with a trigger sensitivity set at 0.5 L/min. Electrocardiogram, intra-arterial blood pressure (radial or femoral artery) and pulse oximetry were monitored throughout the study.
Basic principles of IntelliVent-ASV®
IntelliVent-ASV® is a fully closed-loop control of ventilation and oxygenation available both for passive and active breathing patients.
On the basis of ETCO2 information derived from a mainstream sensor positioned at the Y piece of the ventilator circuit, MV is automatically adjusted to target ranges of ETCO2 between 35 and 41 mmHg. These ETCO2 target ranges can be manually adjusted by users and are more permissive when inspiratory pressure (P INSP) increases above 25 cmH2O. When the MV is automatically adjusted, the combination of V T and RR is determined by the ASV algorithm based on the principle of the least work of breathing previously described [8].
On the basis of SpO2 information derived from a pulse oximetry using a finger or ear probe (Nihon Kohden, Tokyo, Japan), FiO2 and positive end-expiratory pressure (PEEP) are adjusted automatically to keep SpO2 within target ranges of 93 to 97 %. These ranges are adjustable by users and are more permissive when PEEP is above 8 cmH2O. The combination of FiO2 and PEEP is determined by a PEEP–FiO2 table derived from the ARDS Network publications [9, 10] and the user can also adjust the maximum PEEP.
At initiation, a clinician sets the patient’s gender and height and selects the lung condition from ARDS, chronic hypercapnia and/or brain injury. If no lung condition is selected, the patient is considered to have ‘normal lung’. According to the lung condition selected, initial settings of MV, PEEP, FiO2, maximum inspiratory pressure, and target ranges of ETCO2 and SpO2 are determined. Finally, the clinician sets alarm limits. The ventilator then delivers five test breaths, during which SpO2, ETCO2 and expiratory time constant (RCEXP) are measured. Thereafter, closed-loop regulation starts in order to reach the ETCO2 and SpO2 target ranges.
If ETCO2 and SpO2 information are of poor quality or lost, the controllers automatically pause and an alarm is sounded. In addition, FiO2 is automatically increased to 100 % if SpO2 is below 85 %, and 100 % FiO2 manual bypass is still available.
Method
Safety and efficacy of IntelliVent-ASV® were compared with ASV using a crossover design. The two ventilatory modes (ASV and IntelliVent-ASV®) were delivered in random order using the same ventilator (Hamilton Medical S1, Rhazuns, Switzerland), for a period of 2 h with a period of 30 min of ASV with pre-study settings between the two periods. Randomization was applied using numbered sealed envelopes. The initial settings (MV, FiO2 and PEEP) for each period were those selected by the attending clinician at inclusion i.e. the starting settings were the same with both modalities.
Measurements and calculation
Airway pressure and flow were measured using the ventilator’s proximal pneumotachograph (single-use flow sensor, PN 279331, Hamilton Medical, Rhazuns, Switzerland, linear between −120 and 120 L/min with a ±5 % error of measure) inserted between the endotracheal tube and the Y piece. Volume was obtained by integration of the flow signal. V T, RR, P INSP, SpO2 and ETCO2 were continuously monitored and recorded breath by breath for analysis. At the end of each period, arterial blood gases were measured, the static compliance (C STAT) and inspiratory resistances (R INS) were estimated by the least-squares fitting method over the full respiratory cycle [11], and RCEXP was estimated by the V T flow ratio at 75 % of the expiratory V T [12, 13]. P PLAT was measured during a 5-s end-inspiratory occlusion. Bohr dead space and the arterial versus expired CO2 gradient were calculated at the end of each period according to standard formulae [14].
Bedside monitoring
A clinician stayed at the bedside during the entire duration of the study in order to prematurely stop the period if SpO2 decreased below 85 % for more than 2 min, or if V T delivered was over 12 mL/kg PBW for more than 2 min. In addition, the clinician could prematurely end the period and switch to a conventional mode for any clinical reason judged potentially harmful for the patient. In case of interruption for safety reasons during the IntelliVent-ASV® period the patient would be switched to ASV. In case of interruption for safety reasons during the ASV period the patient would be switched to pressure-controlled ventilation.
Statistical methods
The primary goal was safety, estimated by the number of manual switches from IntelliVent-ASV® to ASV or from ASV to pressure control. The secondary goal was to compare ventilation delivered for the two modes. Mean values over the 2-h periods for V T, RR, P INSP, SpO2 and ETCO2 were calculated. Values are expressed as mean ± standard deviation (SD) or median (25–75th interquartile range) when the normality test (Kolmogorov–Smirnov) failed. Median values over the 2-h period for C STAT, R INS, RCEXP, P PLAT and the blood gas analysis were compared using Wilcoxon test. Statistical significance was assumed for p value no greater than 0.05. Statistical analysis was performed using SigmaStat software (version 3.5, SPSS, Inc., Chicago, IL, USA).
Results
Fifty patients were enrolled in the study. Nineteen patients were considered to have normal lung and 31 had acute lung injury (ALI)/ARDS according to the American–European Consensus Conference [15]. Baseline characteristics of the study population are described in Table 1.
There was no safety issue requiring premature interruption of IntelliVent-ASV® as defined in the “Method” section. All patients were able to complete the 2-h periods and none had to be switched to another mode of ventilation. No manual adjustment of PEEP, FiO2 or MV was done during the study periods in any patient.
MV, V T/PBW, RR, P INSP, P PLAT, PEEP and FiO2 were lower during IntelliVent-ASV® as compared to ASV. Respiratory mechanics, pH, PaO2 and PaO2/FiO2 ratio were not different but PaCO2 was slightly higher during IntelliVent-ASV® as compared to ASV. Bohr dead space was lower during IntelliVent-ASV® as compared to ASV (Table 2).
As shown in Fig. 1, during the 2-h period, more breaths had a P INSP below 25 cmH2O, V T/PBW between 6 and 8 mL/kg PBW and SpO2 between 92 and 96 % during IntelliVent-ASV® as compared to ASV (p < 0.05).

Representation of the percentage of breaths in different predefined ranges of values for inspiratory pressure, tidal volume, SpO2 and end-tidal CO2 over the 2-h period in ASV and IntelliVent-ASV®. *p < 0.05 using paired t test
In the 31 patients with ALI/ARDS (Table 3), IntelliVent-ASV® was more permissive in terms of PaCO2 as compared to ASV [46 (37–54) vs. 38 (35–47) mm Hg, respectively, p < 0.001] with similar PaO2/FiO2 ratio at lower PEEP [10 (7–13) vs. 12 (10–15) cmH2O, respectively, p = 0.022], lower FiO2 [34 (30–49) vs. 50 (40–60) %, respectively, p < 0.001] and P PLAT [25 (20–30) vs. 27 (25–30) cmH2O, respectively, p = 0.027]. Figure 2 shows a representative case with automatic adjustment of ventilation and oxygenation parameters.

Changes in minute ventilation (MV), FiO2 and PEEP during adaptive support ventilation (ASV) and IntelliVent-ASV® periods of ca. 30 min in a representative patient (patient #10) with acute lung injury. During the ASV period, there was no change in MV, FiO2 or PEEP. During the IntelliVent-ASV® period, MV decreased progressively from 6.5 to 4 L/min to increase ETCO2 from 33 to 43 mmHg (top panel). FiO2 was initially reduced but SpO2 decreased to 90 %. PEEP and FiO2 were readjusted to finally achieve an SpO2 of 95 % with FiO2 44 % and PEEP 10 cmH2O as compared to FiO2 60 % and PEEP 8 cmH2O with ASV (lower panel)
Discussion
The present study is the first to report the use of a fully closed-loop control of oxygenation and ventilation in ICU patients passively ventilated for acute respiratory failure. The study was designed to assess safety and efficacy of IntelliVent-ASV® and found that over a short period of time IntelliVent-ASV® was safe and delivered ventilation with lower V T/PBW, P INSP, FiO2 and PEEP with similar arterial blood gases results as compared to ASV.
This study has several limitations. First, IntelliVent-ASV® was compared with ASV because it was the default mode used at inclusion for these patients. By using the settings determined by the clinician in charge, the controlled group reflected the ventilation practice in the unit. Interestingly, V T values in the present study (8.3 mL/kg in ASV and 8.1 mL/kg with IntelliVent-ASV®) were very similar to the V T (8.4 mL/kg) observed with volume- or pressure-controlled ventilation in the study by Iotti and co-workers [16]. Finally, we can only speculate on the V T that would have been observed by using volume control or pressure control mode in the controlled group, but most probably they would have been very similar. Second, it was a short-duration safety study. Studying the use of IntelliVent-ASV® over a longer period of time is definitely required and would also give some insight into the impact of IntelliVent-ASV® on clinical outcomes. Third, because it was the first clinical experience of IntelliVent-ASV® in ICU patients, all patients were passive and patients with severe ARDS or high intracranial pressure were not included. These specific populations deserve additional investigation. Fourth, no evaluation of the lung recruitability was performed in the subgroup of ARDS patients.
Closed-loop control ventilation has received a lot of interest over the last decade with the availability of several commercially systems and a growing clinical experience. Up to now, all of the closed-loop systems have focused on the support of the respiratory muscles. IntelliVent-ASV® is the first system to combine an automatic control of ventilation and oxygenation parameters. Such a development is very attractive in many settings but requires strict safety evaluation before clinical use. As it was the first clinical use, we decided to investigate IntelliVent-ASV® in passive and stable patients and to compare it with ASV which is used on a daily basis in our ICU.
The main and important result of the study is that IntelliVent-ASV® was safe in such patients over the study period. There was a careful continuous bedside monitoring by a physician and none of the patients presented any safety issue according to the previously defined criteria.
In addition, during IntelliVent-ASV® the patients had lower V T/PBW and P PLAT as compared to ASV (Table 1). Because the respiratory mechanics (namely RCEXP) were similar during the two periods and the ASV controller is the same in both modes, the decrease in V T/PBW is only explained by the decrease in MV in the IntelliVent-ASV® period. V T values selected in ALI/ARDS patients were not excessively low because their respiratory mechanics were not very disturbed as severe ARDS patients were not included. A more detailed breath by breath analysis over the 2-h period found that more breaths had P INSP less than 25 cmH2O, V T/PBW between 6 and 8 mL/kg PBW and SpO2 between 92 and 96 % during IntelliVent-ASV® as compared to ASV (Fig. 1). These results suggest that closed-loop control of ventilation and oxygenation parameters might help keep ventilation safer than manual settings of ventilation.
A striking result is that IntelliVent-ASV® selected lower MV, V T/PBW, RR, P INSP, P PLAT, PEEP and FiO2 for similar arterial blood gases. We can only speculate on a better ventilation–perfusion matching induced by lower P INSP and V T with IntelliVent-ASV® as compared to ASV. This is sustained by a small but significant decrease in Bohr dead space during the IntelliVent-ASV® period (Tables 2, 3). Assuming no change in the right to left venous admixture (as suggested by a similar PaO2/FiO2 ratio), altogether it suggests a slight reduction in the physiological dead space using IntelliVent-ASV® as compared to ASV. The mechanisms can be only presumptive as the full data on ventilation–perfusion estimated from inert gas or by direct visualization [electric impedance tomography (EIT) or computed tomography (CT) scan] are not available. Interestingly, albeit to be confirmed by a specialized study, it is in the subgroup of ALI/ARDS patients, who are known to have disturbed ventilation/perfusion ratio [17], that more “efficient” ventilation was observed. Adjustments of ventilation (MV, V T/PBW, RR and P INSP) and of oxygenation (FiO2 and PEEP) parameters took place with similar dynamics (data not shown) as the two controllers (oxygenation and ventilation) were both running in parallel. Detailed studies should be done to confirm and to better understand the pathophysiological mechanisms explaining the actual results.
These results also suggest that very often clinicians set parameters that over-assist ventilation and oxygenation. As a consequence, hyperoxia is frequently observed in mechanically ventilated ICU patients [18]. Thus, objectives in terms of PaCO2 or ETCO2 and PaO2 or SpO2 should be revised to avoid unnecessary over-assistance with potential harmful consequences. The use of closed-loop control of ventilation increases the time spent in the desired ventilation zone [19, 20] and may help clinicians to revise the objectives. Such closed-loop systems may in theory be able to work with other modes of ventilation, for instance pressure support ventilation (PSV) or volume assist controlled ventilation with closed-loop control of FiO2 and PEEP. In the present case, having ASV in the “background” provided additional functional and safety features such as automatic adjustment of V T and RR within the previously described safety framework [8].
If confirmed by long-term studies the present results may have significant clinical implications. ICUs today are facing an increase in the number of patients to treat, in parallel with an increase in the severity and complexity of such patients. On the other hand, a shortage of resources [21, 22], burnout problems in the caregivers [23] and training difficulties have been evidenced in many countries [24]. Quality and safety should also improve in order to decrease workload, hospital duration, morbidity, mortality and costs. Automatic ventilation may be part of a multifaceted strategy to help solve this complex equation.
The algorithms that drive IntelliVent-ASV® are based on expert knowledge for the ventilation and oxygenation controllers and on physiology for the determination of V T–RR combination. For normal-lung patients, the ventilation parameters selected automatically by IntelliVent-ASV® were very similar to our usual manual settings in ASV (data not shown). In ALI/ARDS patients, IntelliVent-ASV® was able to select lower settings (MV, P INSP, V T, FiO2…) than clinical practice with the same or improved gas exchange results. The automatic decrease in settings (de-escalation) may have an impact on other therapeutic aspects such as sedation. As a result of the diversity of patients treated in ICU, one algorithm may not fit all patients however. The most severe and unstable patients, or very specific patients in which recommendations should be tuned, will still require an individualized medical expertise at the bedside.
In conclusion, this randomized crossover study comparing IntelliVent-ASV® with ASV for 2-h periods in passive patients with acute respiratory failure found that IntelliVent-ASV® was safe and associated with lower P INSP, P PLAT, PEEP, V T/PBW and similar PaO2/FiO2 ratios. IntelliVent-ASV® needs to be studied over longer periods of time and compared with conventional modes with clinical outcome assessments.
References
Chatburn R, Mireles-Cabodevila E (2011) Closed-loop control of mechanical ventilation: description and classification of targeting schemes. Respir Care 56:85–98
Wysocki M, Brunner JX (2007) Closed-loop ventilation: an emerging standard of care? Crit Care Clin 23:223–240
Arnal JM, Wysocki M, Nafati C, Donati SY, Granier I, Corno G, Durand-Gasselin J (2008) Automatic selection of breathing pattern using adaptive support ventilation. Intensive Care Med 34:75–81
Sulemanji D, Marchese A, Garberini P, Wysocki M, Kacmarek R (2009) Adaptive support ventilation: an appropriate mechanical ventilation strategy for acute respiratory distress syndrome? Anesthesiology 111:863–870
Gruber PC, Gomersall CD, Leung P, Joynt GM, Ng SK, Ho KM, Underwood MJ (2008) Randomized controlled trial comparing adaptive-support ventilation with pressure-regulated volume-controlled ventilation with automode in weaning patients after cardiac surgery. Anesthesiology 109:81–87
Kirakli C, Ozdemir I, Zeren Ucar Z, Cimen P, Kepil S, Ozkran SA (2011) Adaptive support ventilation for faster weaning in COPD: a randomized controlled trial. Eur Respir J 38:774–780
Chen CW, Wu CP, Dai YL, Perng WC, Chian CF, Su WL, Huang YC (2011) Effect of implementing adaptive support ventilation in a medical intensive care unit. Respir Care 56:976–983
Tassaux D, Dalmas E, Gratadour P, Jolliet P (2002) Patient-ventilator interactions during partial ventilatory support: a preliminary study comparing the effects of adaptive support ventilation with synchronized intermittent mandatory ventilation plus inspiratory pressure support. Crit Care Med 30:801–807
Acute Respiratory Distress Syndrome Network (2000) Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 342:1301–1308
Acute Respiratory Distress Syndrome Network (2004) Higher versus lower positive end-expiratory pressures in patients with acute respiratory distress syndrome. N Engl J Med 351:327–336
Iotti GA, Braschi A, Brunner JX, Smits T, Olivei M, Palo A, Veronesi R (1995) Respiratory mechanics by least squares fitting in mechanically ventilated patients: applications during paralysis and during pressure support ventilation. Intensive Care Med 21:406–413
Brunner JX, Laubsher TP, Banner MJ, Iotti G, Brashi A (1995) Simple method to measure total expiratory time constant based on passive expiratory flow-volume curve. Crit Care Med 23:1117–1122
Lourens MS, Van Den Berg B, Aerts JG, Verbraak AFM, Hoogsteden HC, Bogaard JM (2000) Expiratory time constants in mechanically ventilated patients with and without COPD. Intensive Care Med 26:1612–1618
Lucangelo U, Blanch L (2004) Dead space. Intensive Care Med 30:576–579
Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M, Le Gall JR, Morris A, Spragg R (1994) Report of the American-European Consensus Conference on acute respiratory distress syndrome: definitions, mechanism, relevant outcomes, and clinical trial coordination. Consensus Committee. Am J Respir Crit Care Med 149:818–824
Iotti G, Polito A, Belliato M, Pasero D, Beduneau G, Wysocki M, Brunner J, Brashi A, Brochard L, Mancebo J, Richard JC, Slutsky A (2010) Adaptive support ventilation versus conventional ventilation for total ventilatory support in acute respiratory failure. Intensive Care Med 36:1371–1379
Ware L, Matthay M (2000) The acute respiratory distress syndrome. N Engl J Med 342:1334–1349
De Graaff AE, Dongelmans DA, Binnekade JM, De Jonge E (2011) Clinician’s response to hyperoxia in ventilated patients in a Dutch ICU depends on the level of FiO2. Intensive Care Med 37:46–51
Dojat M, Harf A, Touchard D, Lemaire F, Brochard L (2000) Clinical evaluation of a computer-controlled pressure support mode. Am J Respir Crit Care Med 161:1161–1166
Lellouche F, Bouchard PA, Laubsher T, Blackburn S, L’Her E, Wysocki M (2010) Prospective randomized controlled study comparing conventional ventilation versus a fully close loop ventilation (IntelliVent®) in post cardiac surgery ICU patients. Intensive Care Med 36:S752
Constantin JM, Leone M, Jaber S, Allaouchiche B, Orban JC, Cannesson M, Fourcade O, Morel J, Martin C, Lefrant JY, AzuRéa (2010) Activity and the available human resources working in 66 French Southern intensive care units. Ann Fr Anesth Reanim 29:512–517
Tarnow-Mordi WO, Hau C, Warden A, Shearer AJ (2000) Hospital mortality in relation to staff workload: a 4-year study in an adult intensive-care unit. Lancet 356:185–189
Embriaco N, Papazian L, Kentish-Barnes N, Pochard F, Azoulay E (2007) Burnout syndrome among critical care healthcare workers. Curr Opin Crit Care 13:482–488
Parkes J, Hyde C, Deeks J, Milne R (2001) Teaching critical appraisal skills in health care settings. Cochrane Database Syst Rev CD001270
Acknowledgments
This study was sponsored by Hamilton Medical. J.-M. Arnal was supported by Hamilton Medical in presenting the results at international conferences.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was conducted in the Intensive Care Unit of Font Pré Hospital, Toulon, France.
Rights and permissions
About this article
Cite this article
Arnal, JM., Wysocki, M., Novotni, D. et al. Safety and efficacy of a fully closed-loop control ventilation (IntelliVent-ASV®) in sedated ICU patients with acute respiratory failure: a prospective randomized crossover study. Intensive Care Med 38, 781–787 (2012). https://doi.org/10.1007/s00134-012-2548-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-012-2548-6