
Abstract
Objective
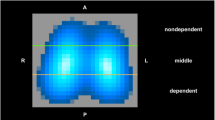
The purpose of lung recruitment manoeuvres is to open collapsed lung regions, improve gas exchange and optimise regional lung mechanics. This study investigates the efficacy of recruitment manoeuvres for improving regional ventilation distribution as characterised using electrical impedance tomography (EIT).
Design, subjects, interventions
A ventilated ovine smoke inhalation lung injury model was used. Respiratory mechanics and regional filling capacity of the lung were measured using EIT pre- and post- recruitment and compared to a control group.
Measurements
EIT, expressed as the time course relation of the regional versus the global impedance change, measured the regional filling capacities of the lung.
Main results
After smoke inhalation injury, the dependent lung showed a significantly larger area of collapse and a reduced filling capacity compared to the non-dependent lung. After recruitment the ventilated volume increased and the dependent lung showed improved respiratory mechanics, whereas the non-dependent lung was more likely to be hyper-inflated during tidal breathing.
Conclusions
Lung recruitment manoeuvres have a significant impact on regional lung mechanics and individual measurement of ventilation distribution using EIT may assist to improve ventilatory management.
Similar content being viewed by others

Introduction
The principal objective of ventilatory management is the maintenance of adequate gas exchange whilst minimising iatrogenic lung damage [1]. The key elements of such a protective approach are to limit lung distension and to maintain sufficient end-expiratory volume to prevent alveolar collapse [2, 3]. One dilemma of current ventilation strategies is that the injured lung behaves as a multi-compartment model, while the ventilator delivers support assuming a single compartment model.
Pressure–volume (PV) curves have been used for titration of ventilatory support, to improve outcomes and reduce ventilator induced lung injury. Unfortunately, the PV curve obtained from the whole lung merely gives a composite picture of a heterogeneous lung, and is not representative of the respiratory mechanics of regional lung compartments [4, 5]. Differences in regional alveolar opening pressures and potential regional hyperinflation can be assessed using CT scanning of the lung.
Electrical impedance tomography (EIT) has been used to measure global and regional ventilation distribution [6]. Regional visco-elastic properties of the lung have been described using regional pressure–impedance curves [7]. EIT has further been used to describe cyclic closing and reopening of different lung regions in a heterogeneous group of patients with acute respiratory distress syndrome (ARDS) [8]. To investigate regional differences in lung mechanics we have used a smoke inhalation ARDS model. Smoke provokes significant ventilation inhomogeneity with the dependent lung commonly more affected by the smoke inhalation injury. Hence, regional differences in lung mechanics were expected and the validity of EIT as a bedside lung function monitoring tool to detect these regional differences could be tested. We aimed to demonstrate in this standardised lung injury model that significant intra-individual differences exist in regional lung mechanics.
Methods
Study design
Fifteen Merino ewes were randomly allocated into three groups with five animals each:
-
PEEP trial recruitment group (Group A)
-
Deflation–Reinflation recruitment group (Group B)
-
Control group (Group C).
The smoke induced lung injury was allowed to develop for a period of 2 h before recruitment manoeuvres were performed. No recruitment manoeuvre was performed in the control group.
Details of ventilatory management, smoke inhalation model, recruitment manoeuvres and physiological measurements are given in the supplementary material accompanying the paper.
EIT data
EIT data was obtained using the Goettingen GoeMF II system (Viasys Healthcare, Amsterdam, The Netherlands) at a sampling rate of 13 Hz and analysed offline using purpose written software (Matlab 7.1).
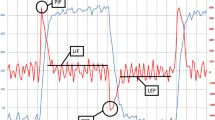
The regional tidal volume change was compared to global tidal volume change by plotting the impedance change of the region of interest against that of the global signal forming a curve. This comparison of regional versus global impedance change represents the lag or lead in regional filling. If a region filled slower than the rest of the lung during the initial phase of the inspiration, tidal recruitment may have occurred. In contrast a region may have filled faster than the rest of the lung and regional tidal hyperinflation may have occurred. Ideally all regions fill in absolute synchrony, a scenario referred to as protective ventilation.
The slope of the mentioned curve was then calculated using the following equation:
where I(g) is the impedance, FI filling index in a region of interest, a and c are constants. An FI <1 indicates tidal hyperinflation, a FI >1 tidal recruitment and FI = 1 protective ventilation.
Respiratory mechanics including respiratory compliance, resistance and stress index were measured. The details and results of these techniques are described in the supplement.
Results
Filling characteristics
The FI values prior to smoke inhalation were >1 in the right lung and <1 in the left lung; 120 min after smoke inhalation, the FI of the right lung increased whereas that of the left lung remained relatively unchanged (Fig. 1).

Filling indices per slice from right to left of the lung for all measured animals pre, post smoke inhalation and post lung recruitment. Values >1 indicate tidal recruitment and values <1 indicate tidal hyperinflation. Mean and CI are given in the graph
The confidence intervals increased after smoke inhalation and those for the right lung were larger than for the left lung, reflecting the heterogeneous nature of the smoke inhalation injury.
Figure 1 shows the FI values measured at 30, 120 and 240 min post lung recruitment in group A, B and control. In group A the dependent lung initially showed tidal recruitment after the recruitment manoeuvre but this effect disappeared after 240 min. In group B there was initially a large degree of tidal recruitment in the dependent lung, this dissipated and after 120 min, more tidal recruitment had occurred in the central to non-dependent lung, until finally after 240 min, the dependent lung once again showed greater tidal recruitment. The control group exhibited less variation than the two recruitment groups with only minor changes in the FI values during the observation period.
Additional results for respiratory mechanics are given in the supplementary material accompanying the paper.
Discussion
We demonstrated in an experimental smoke inhalation lung injury model that recruitment has a very individual impact on regional lung mechanics. The regional filling characteristics measured with electrical impedance tomography were heterogeneously distributed throughout the lung warranting individual assessment of respiratory mechanics for optimal titration of ventilatory support.
The gas delivered by the ventilator follows the path of least resistance and highest compliance; hence, lung regions less affected by the disease process will be better ventilated and are potentially at risk of barotrauma [9].
Current best practice for respiratory support employs lung recruitment manoeuvres to open previously collapsed lung compartments thus enabling their participation in gas exchange. This allows ventilation of a larger lung volume whilst minimising the risk of tidal hyperinflation of less diseased lung regions.
Regional filling characteristics of the lung
Using the plot of regional versus global impedance change the time lag or lead between regional and global filling can be measured. If one region of the lung fills slower than the rest of the lung during inspiration, and so lags behind it, “tidal recruitment” may be occurring. In contrast a region may fill faster, or lead, the rest of the lung indicating the possible presence of tidal hyperinflation. Ideally if a region fills in synchrony with the rest of the lung, protective ventilation may be occurring. The filling capacities of the different regions in our study were reported from dependent right to the non-dependent left lung as the ewes were kept in a right lateral position. Prior to smoke inhalation the right lung was characterised by possible tidal recruitment (FI <1) whereas the non-dependent (left) lung showed possible tidal hyperinflation (FI >1). These results confirmed that, using a relatively low PEEP of 5 cm H2O, the dependent lung is more likely to be ventilated near the closing capacity during mechanical ventilation.
The dependent lung received more ventilation than the non-dependent lung, hence a greater proportion of the smoke administered, and the greatest change in measured EIT parameters.
The confidence intervals of the parameters obtained from the dependent lung increased significantly after smoke inhalation, indicating that the smoke induced injury caused very heterogeneous lung damage and that regional respiratory mechanics need to be assessed for each subject separately.
Impact of lung recruitment on regional filling capacity
There was high inter-subject variability found after the recruitment manoeuvres. In general the measured FI were >1 in the dependent lung whereas in the control group the calculated FI values were ≤1. In the non-dependent lung the changes in regional mechanics were less marked in the recruitment groups, reflecting the reduced impact of the recruitment manoeuvres on the non-dependent lung.
Regional ventilation distribution after lung recruitment
Using EIT monitoring it was seen that the effect of lung recruitment remained significant for 4 h after the manoeuvre whereas an effect was not noticeable using conventional respiratory mechanics.
Limitations of the study
Inter-subject variability of the EIT parameters were significantly greater post smoke or post recruitment compared to pre smoke. As such, further studies with more animals are warranted.
Clinical significance of the study
Our study demonstrated that individual monitoring of regional lung mechanics using EIT is feasible and the effect of lung recruitment can be reliably assessed. There is a need for further outcome studies to investigate whether individual titration of ventilatory support improves lung mechanics and outcome in clinical settings.
Conclusion
This pilot study has shown that a very heterogeneous lung injury can be created using smoke inhalation. Lung recruitment manoeuvres were shown to have a very heterogeneous impact on regional lung recruitment. Hence, individual assessment of respiratory mechanics using EIT or a similar imaging technique for optimal titration of ventilatory support is warranted.
References
Hickling KG, Walsh J, Henderson S, Jackson R (1994) Low mortality rate in adult respiratory distress syndrome using low-volume, pressure-limited ventilation with permissive hypercapnia: a prospective study. Crit Care Med 22:1568–1578
Amato MB, Barbas CS, Medeiros DM, Schettino Gde P, Lorenzi Filho G, Kairalla RA, Deheinzelin D, Morais C, Fernandes Ede O, Takagaki TY et al (1995) Beneficial effects of the “open lung approach” with low distending pressures in acute respiratory distress syndrome. A prospective randomized study on mechanical ventilation. Am J Respir Crit Care Med 152:1835–1846
Amato MB, Barbas CS, Medeiros DM, Magaldi RB, Schettino GP, Lorenzi-Filho G, Kairalla RA, Deheinzelin D, Munoz C, Oliveira R, Takagaki TY, Carvalho CR (1998) Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome (comment). N Engl J Med 338:347–354
Puybasset L, Gusman P, Muller JC, Cluzel P, Coriat P, Rouby JJ (2000) Regional distribution of gas and tissue in acute respiratory distress syndrome. III. Consequences for the effects of positive end-expiratory pressure. CT Scan ARDS Study Group. Adult respiratory distress syndrome. Intensive Care Med 26:1215–1227
Rouby JJ, Puybasset L, Cluzel P, Richecoeur J, Lu Q, Grenier P (2000) Regional distribution of gas and tissue in acute respiratory distress syndrome. II. Physiological correlations and definition of an ARDS Severity Score. CT Scan ARDS Study Group. Intensive Care Med 26:1046–1056
Frerichs I, Hinz J, Herrmann P, Weisser G, Hahn G, Dudykevych T, Quintel M, Hellige G (2002) Detection of local lung air content by electrical impedance tomography compared with electron beam CT. J Appl Physiol 93:660–666
Hinz J, Moerer O, Neumann P, Dudykevych T, Frerichs I, Hellige G, Quintel M (2006) Regional pulmonary pressure volume curves in mechanically ventilated patients with acute respiratory failure measured by electrical impedance tomography. Acta Anaesthesiol Scand 50:331–339
Hinz J, Gehoff A, Moerer O, Frerichs I, Hahn G, Hellige G, Quintel M (2006) Regional filling characteristics of the lungs in mechanically ventilated patients with acute lung injury. Eur J Anaesthesiol 24:414–424
Gattinoni L, Pesenti A (2005) The concept of “baby lung”. Intensive Care Med 31:776–784
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Grant, C.A., Fraser, J.F., Dunster, K.R. et al. The assessment of regional lung mechanics with electrical impedance tomography: a pilot study during recruitment manoeuvres. Intensive Care Med 35, 166–170 (2009). https://doi.org/10.1007/s00134-008-1324-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-008-1324-0