
Abstract
Background
Acute respiratory distress syndrome (ARDS) is the most severe manifestation of acute lung injury (ALI). In patients who survive the acute injury the process of repair and remodelling may be an independent risk factor determining morbidity and mortality. This review explores recent advances in the field of fibroproliferative ARDS/ALI, with a special emphasis on (a) the primary contributing factors with a focus on cellular and soluble factors, and (b) mechanisms involved in repair and remodelling as they pertain to the importance of cell death, re-population, and matrix deposition.
Discussion
Factors influencing progression to fibroproliferative ARDS vs. resolution and reconstitution of the normal pulmonary parenchymal architecture are poorly understood. Determinants of persistent injury and abnormal repair and remodelling may be profoundly affected by both environmental and genetic factors. Moreover, cumulative evidence suggests that acute inflammation and fibrosis may be in part independent and interactive processes that are autonomously regulated and thus amenable to individual and specific therapy.
Conclusions
Although our current understanding of these processes is limited by the inability to accurately replicate the complex human physiology in laboratory settings, it has recently become apparent that the process of repair and remodelling begins early in the course of ARDS/ALI and may be determined by the type of pulmonary injury. Understanding the mechanisms leading to and regulating fibroproliferative changes may contribute to the development of novel early therapeutic interventions in ARDS/ALI patients.
Similar content being viewed by others


Introduction
Acute respiratory distress syndrome (ARDS), the most severe manifestation of acute lung injury (ALI), is typically described as a stereotyped response to lung injury with transition from alveolar capillary damage to a fibroproliferative phase, independent of initial cause [1]. Most ARDS patients survive the acute initial phase of lung injury and progress to either reparation of the lesion or evolution of the syndrome [2]. Despite advances in the management of ARDS, mortality remains high (40%). For those patients who die extended pulmonary fibrosis is seen in 55% at autopsy, suggesting that dysregulated repair may contribute to the morbidity and mortality in these patients. The factors determining whether pulmonary fibrosis or restoration of the normal pulmonary architecture occur in ARDS remain unknown. Moreover, the processes characterizing lung injury and repair are modulated by ongoing external pro-injurious or anti-injurious stimuli (e. g. ongoing infection or/and resuscitation) and are a result of genetic factors. Repetitive biochemical and biophysical stimuli not only play a role in the natural history of ALI/ARDS but, when treated, can lead to improved clinical outcomes. Although acute and persistent inflammation is a critical determinant of fibroproliferative changes in the lung, multiple lines of evidence, suggest that the fibrotic process may be (in part) an independent risk factor that is autonomously regulated, and thus amenable to separate therapy [3–5].
Recent reviews have eloquently addressed the development of fibroproliferation in ALI/ARDS [3–6]. This contribution presents an abbreviated overview of recent advances in the understanding of (a) the primary factors contributing to the development of fibroproliferation with a focus on cellular and soluble factors and (b) mechanisms involved in repair and remodelling, especially as they pertain to the importance of cell death, re-population and matrix deposition. Current understanding of these processes is limited by the inability to accurately replicate the complex human physiology in laboratory settings.
Inflammation and fibroproliferation
Until recently the natural history of fibroproliferative ARDS had been described as developing over three distinct phases: an inflammatory or exudative, a proliferative and a fibrotic phase. Recently, however, it has become apparent that the process of fibrosing alveolitis begins early in the course of ARDS [7, 8]. Transcriptional responses in ALI genes involved in inflammation and repair are differentially expressed simultaneously very early in the course of injury [9], and many mediators are common to both processes. This paradigm shift in our understanding of injury and repair is further supported by evidence that patients with well known chronic fibrotic lung disorders have persistently elevated levels of acute injury related cytokines and chemokines in alveolar lavage samples [10, 11]. Conversely, factors previously thought to be primarily involved in chronic phases of lung injury such as transforming growth factor (TGF) β, have been shown to mediate acute injury, specifically acute pulmonary oedema in ALI [12]. Figure 1 is a schematic representation of processes resulting in fibrosis, underscoring co-regulation, as opposed to sequential regulation of these processes.

Schematic of dysregulated repair. Hypothetical scheme of molecular mechanisms of fibroproliferation in ALI/ARDS. Persistent and exaggerated inflammation occurs secondary to either unresolved inflammation or/and repeated injury or alveolar epithelial cell activation. This is modulated by non-modifiable risk factors for fibroproliferation such as age, gender and genetic susceptibility. Inflammatory and parenchymal cells release factors inducing fibroblast migration and proliferation and changes in cell phenotype (myofibroblasts). The microenvironment of the injured lung lead to alveolar epithelial cell drop-out (apoptosis and/or necrosis), resulting in loss of normal function. The provisional matrix contributes to ongoing phenotypic changes in cells involved in the repair system and in the presence of profibrotic stimuli irreversible changes in extracellular matrix architecture occurs resulting in erratic remodelling of the lung parenchyma, resulting in a gain of abnormal function
Optimal repair requires that a provisional fibrin matrix on the basement membrane provide a platform for cell adhesion, spreading, and migration. In pathological fibrosis, provisional matrices formed in the context of injury persist, emitting signals to activate an inflammatory response leading to relentless fibroblast migration and proliferation and to expansion of connective tissue elements leading to permanent matrix remodelling. Disordered repair is characterized by impaired fibrinolysis of the inflammatory coagulum, fibrocellular proliferation, impaired angiogenesis and distortion of the lung parenchyma. Intra-alveolar fibrosis (remodelling) results in alveolar obliteration, and ultimately loss of functional alveolar capillary units. In this context, resulting persistent respiratory failure secondary to progressive fibrosis is associated with poor prognosis [13].
Primary contributing factors to repair and remodelling in ALI/ARDS
Cellular component
Parenchymal cells: epithelial, endothelial and fibroblasts
Repair is the process of ‘replacing injured tissue by regenerating native parenchymal cells and filling in defects with fibroblast tissue’ [14]. Diffuse alveolar damage with denudation of the alveolar membrane is characteristic of ARDS. Efficient alveolar epithelial repair may reduce the development of fibrosis, since the presence of an intact alveolar epithelial layer suppresses fibroblast proliferation and matrix deposition. Impaired or delayed re-epithelialization may result from loss of proliferative capacity, altered apoptosis or ineffective migration and differentiation of alveolar cells and their progenitors. Epithelial repair involves close coordination and interaction between the alveolar type II cell (AT-II) and various cell types, including mesenchymal cells, endothelial cells (EC) as well as the extracellular matrix, which may coordinate by a variety of soluble mediators released into the alveolar space the process of re-epithelialization [5].
The importance of the alveolar epithelium as a primary mediator of fibroproliferation after ALI can be inferred from studies of bleomycin induced lung injury. In this model failure to express the integrin αvβ6 (adhesion molecule that binds matrix, anchors cells and activates TGF-β) confers almost complete protection against bleomycin induced lung injury and fibrosis in mice [15]. Similarly, the function of the endothelium has been inferred from experiments exploring the role of cyclo-oxygenase (COX) 2 derived eicosanoids in pulmonary fibrosis, where mutations in the ligand receptor pair prostacyclin and its receptor derived from ECs confers susceptibility to bleomycin induced lung injury and fibrosis [16].
Ineffective repair and pathogenic fibrosis has also been explained by ‘loss of function’ due to increased rates of alveolar epithelial cell ‘dropout’ resulting from apoptotic or necrotic death after severe alveolar membrane denudation. Epithelial drop-out has been implicated in the other forms of chronic fibroproliferative lung disorders. Interestingly, not only necrosis but epithelial apoptosis has been associated with the development of pulmonary fibrosis [17]. The role of EC apoptosis is much less understood, although endothelial functional drop-out has been implicated as a trigger for fibrosis in scleroderma [18].
In addition to the loss-of-function, the ‘gain-of-function’ associated with abnormal fibroblast repopulation may be important. Fibroblasts from fibroproliferative lesions can display an enhanced proliferative phenotype independent of continuous exogenous stimulation [19]. Recently Horowitz et al. [19] isolated and characterized a novel population of mesenchymal cells from ARDS patients. Cells isolated from patients with persistent or nonresolving ARDS had an enhanced activational profile characterized by enhanced prosurvival signalling and an antiapoptotic phenotype. These findings support the concept that apoptosis of mesenchymal cells is an essential component of normal repair and resolution of ARDS and suggest that dysregulation of this process contributes to persistent ARDS. Figure 2 illustrates the contribution of key cell types to the fibroproliferative process.

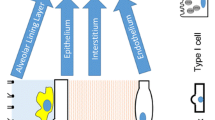
Important contributors to the development of fibroproliferative ARDS. Progressive fibroproliferation results from dynamic alterations in the alveolar microenvironment that eventually promotes loss of alveolar epithelial cells and accumulation of activated fibroblasts/myofibroblasts. These alterations include the presence of or activation of profibrotic cytokines, growth factors and chemokines; eicosanoid imbalance with relative deficiency in PGE2; impaired fibrinolysis; overproduction of tissue inhibitors of metalloproteinases (TIMPs) relative to matrix metalloproteinases (MMPs); and a state of elevated oxidative stress. Key cell types contribute to this process including parenchymal cells (epithelial, endothelial and fibroblasts) and myeloid derived cells (macrophages, neutrophils and lymphocytes). IL8, interleukin 8; TNFα, tumour necrosis factor α; PDGF, platelet-derived growth factor; EGF, epithelial growth factor; TGFβ, transforming growth factor β; TGFα, transforming growth factor α; PGE 2, prostaglandin E2; IL-RA, interleukin receptor antagonist; PGI 2, prostacyclin; ICAM, intracellular adhesion molecule; IL4, interleukin 4; IFNγ, interferon γ; IGF, insulin-like growth factor; IL-1β, interleukin 1β; Th1, T-helper cell type 1 responses; Th2, T-helper cell type 2 responses. Adapted from Ref. [6]
Epithelial injury and re-epithelialization
Key features of the alveolar remodelling process during recovery from injury are AT-II cell migration, proliferation and regeneration, which rapidly reseal the denuded alveolar surface. Recent experiments suggest that signalling pathways important in lung remodelling, repair and regeneration after ALI recapitulate respiratory ontogeny [20]. Presumably, after injury normally quiescent AT-II cells transiently regain the capacity to proliferate and express numerous cell cycle related genes, as well as secrete and activate matrix metalloproteases—fundamental enzymes for digestion of the basement membrane. Transdifferentiation of epithelial cells into matrix producing fibroblasts and myofibroblasts with enhanced matrix turnover has been suggested as a mechanism for remodelling after injury. At least two pathways initiated by key mediators of epithelial and mesenchymal cell cross-talk during embryonic airway morphogenesis have been implicated in ALI. The first is sonic hedgehog (SHH), which promotes proliferation of neuroendocrine cells in airway epithelium and has been demonstrated to be activated within the airway epithelium during repair of acute airway injury [21]. The second is related to β-catenin [22], a central regulatory protein in the Wnt cascade which controls temporal and spatial pulmonary morphogenesis.
Another important process involved in the reconstitution of alveolar membrane is cellular regeneration. Until recently this was thought to occur from resident epithelial progenitor cells located at the base of submucosal glands and ducts that differentiate into airway epithelial cells [23]. These cells express markers of early epithelial differentiation such as cytokeratins 5 and 14 [24]. Under homeostatic conditions there are a sufficient number of resident progenitor cells to replace the continuous loss of airway epithelial cells. However, after significant injury the ability of local cells to reconstitute the denuded epithelium is overwhelmed and circulating progenitor cells are recruited to areas of injury to contribute to repair. It has been proposed that bone marrow stromal cells have the potential to differentiate into lung epithelial cells [25, 26]. Bone marrow mesenchymal cells have been shown to form pulmonary epithelial cells of both proximal and distal airways [27]. Transfer of bone marrow derived mesenchymal stem cells may protect the lung against bleomycin-induced lung injury [28]. Recently the first set of experimental evidence demonstrating that CK5+ bone marrow derived progenitor cells are recruited to the airway epithelium in response to injury was presented by Gomperts et al. [29]; homing signals promoting recruitment to sites of injury appear to depend upon interaction between the CXCR4 receptor and the ligand CXCL12.
The role of apoptosis in repair and remodelling
Studies indicate that apoptosis contributes to the pathogenesis of lung fibrosis as well as to its resolution [30]. Apoptosis can be detrimental or beneficial, depending on the cell type, the circumstances and the timing. While myofibroblast and inflammatory cell apoptosis might be beneficial [31], excessive AT-II cell apoptosis could lead to the destruction of alveolar septa and loss of the ‘scaffolding’ intended for alveolar repair.
The notion that AT-II cell apoptosis is involved in the initiation and/or progression of fibrotic lung disease is supported by various experimental animal models of fibrosis [32]. Apoptotic epithelial cells can be found in the damaged alveolar epithelium of patients with ARDS [33]. In the resolution phase apoptosis of type II pneumocytes largely responds to the disappearance of excess epithelial cells. The Fas ligand mediated apoptosis pathway has been the main apoptotic mechanism implicated in AT-II cell death. Bronchoalveolar lavage (BAL) fluid from patients with ARDS contains elevated concentrations of membrane bound and soluble Fas ligand (sFasL); and pneumocytes from patients with ALI/ARSD express sFasL and membrane bound Fas, suggesting that the Fas system plays a role in ARDS/ALI related apoptosis [34]. Angiotensin II (ANG II) appears to induce AT-II cell apoptosis by this pathway [35]. TGF-β has also been shown to induce Fas-ligand mediated apoptosis of AT-II cells [36].
Apoptosis of epithelial cells and neutrophils are interrelated events. Apoptosis of myeloid cells probably plays an important role in attenuating lung injury and may ultimately benefit the outcome of patients with ARDS [37]. In response to Fas ligand or tumuor necrosis factor (TNF) α, bronchiolar epithelial cells undergo apoptosis and secrete interleukin (IL) 8 and nuclear factor (NF) κB, which in turn suppresses the apoptosis of neutrophils, increasing lung injury. The alveolar epithelium is one of the primary target of Fas-mediated apoptosis in ALI [38].
The activated neutrophil and its by-products
Neutrophil infiltration is the hallmark of acute inflammation. Excessive quantities of neutrophil products including elastase, collagenase, reactive oxygen species, and cytokines are present in patients with ARDS. Blocking antibodies to adhesion molecules, notably β2 integrins, demonstrates that while neutrophil migration still occurs injury is reduced. The presence of neutrophils however, is not absolutely required for the development of ALI; this can occur in neutropenic patients [39] and in animal models of lung injury after neutrophil depletion [40]. During the repair process neutrophils recruited to the site of injury may contribute to host defence and injury, and to the repair process itself. Few studies have addressed the development of pulmonary fibrosis in the absence of neutrophils. In neutrophil-depleted bleomycin-treated hamsters collagen synthesis is enhanced [41], suggesting a role for neutrophils in membrane repair and remodelling. Recently neutrophil defensins have been implicated in wound repair. In vitro studies demonstrated that neutrophil defensins enhance proliferation of human lung epithelial [42] and epithelial wound closure [43].
Neutrophil elastases are involved in destroying ECs. Soluble cadherins (an endothelial junction protein) have been identified in the serum of ARDS patients, suggesting an elastase-mediated proteolysis of the EC and disruption of the EC junction. This is further supported by the presence of thrombomodulin (an EC surface anticoagulant protein) in the serum of patients with ARDS, indicating the proteolytic release of an EC membrane protein [44]. Moreover neutrophil elastases are clearly involved in mucin biogenesis (key glycoproteins in airway health and disease). Although this glycoprotein has been shown to play an important role in chronic lung diseases, few studies have addressed mucin production in ARDS. Serum levels of mucin have been reported to be at least 20 times that of patients with other chronic inflammatory lung diseases [45], suggesting that the activity of neutrophil elastases extend much beyond simple proteolytic activity. Exaggerated mucin production may contribute to airway obstruction and remodelling by mucus and consequent high morbidity and mortality associated with chronic fibroproliferative and inflammatory lung diseases [46]. In a single study serial measurements of serum mucin levels in ARDS patients were inversely correlated with static respiratory system compliance and P:F ratio (measurement of oxygenation) and positively correlated with lung injury scores [45].
Mononuclear phagocytes
Macrophages have been thought to be important in the progression of ALI to fibroproliferative ARDS as they are present in high numbers and release a variety of mediators and growth factors that act as potent mitogens and chemotractants for fibroblasts and smooth muscles cells resulting in a dramatic proliferative response in these cell types [47]. After lung injury alveolar macrophages are found in contact with alveolar epithelial cells in the alveolar space while circulating monocytes are contained within the vascular space in contact with ECs. Alveolar macrophages secrete numerous proinflammatory mediators (IL-1β, IL-4 and IL-13) and growth factors TGF-β, TGF-α, platelet-derived growth factor, fibroblast growth factor, insulin-like growth factor I, and other epidermal growth factor-like molecules. These peptide growth factors influence mesenchymal cell migration, proliferation and extracellular matrix deposition, thus implicating them in the progression of fibroproliferative lung disorders [48]. Moreover, alveolar macrophages are significantly activated after ventilator-induced lung injury, and they have been shown to be a source of ongoing inflammatory mediators in response to it [49]. The precise role of macrophages in ALI, however, is not well defined. Recent papers have shown that pharmacological depletion of alveolar macrophages may lead to deterioration in pulmonary injurious parameters [50, 51]. These studies suggest a potential role for these cells in lung protection or repair.
In contrast to alveolar macrophages, little is known about the role of circulating monocytes in fibroproliferation. Monocytes rapidly marginate to the lungs after induction of pulmonary injury in animal models of ALI [52]. Injection of activated wild-type donor leucocytes to wild-type or TNF-α receptor double knockout (deficient in R1 and R2) recipients demonstrate that lung-marginated monocytes can induce TNF-dependent upregulation of adhesion molecules on pulmonary endothelial cells. Injection of activated donor leukocytes from TNF-α knock-in mice that express uncleavable mutant membrane TNF-α also induced adhesion molecule upregulation in wild-type recipients without a systemic soluble TNF release. These results reveal a potential role for cell–cell mediated regulation of pulmonary microcirculation in inflammation, and possibly in repair during ALI [53].
Soluble component
IL-1β
The role of IL-1β in fibroproliferative ARDS remains controversial. On one hand, BAL from patients with early ALI has increased IL-1β dependent mitogenic effect on cultured fibroblasts [54] and induces collagen synthesis (collagen types I and III). On the other, it is involved in inhibiting fibroblast proliferation by inducing prostaglandin E2 (PGE2) [55]. The secretion of PGE2 can also be in part induced by IL-1 receptor antagonist (IL-1Ra) [56]. IL-1Ra is a naturally occurring antagonist of IL-1β and has been associated with a number of fibroproliferative diseases and wound healing [57]. Elevated levels of IL-1Ra may attenuate IL-1β bioactivity during the pathogenesis of other diseases of matrix remodelling thus presumably creating a local environment that favours fibroproliferation and matrix deposition [58]. Absence of IL-1Ra may lead to impaired wound healing and reciprocal suppression of TGF-β signal pathway, impairing collagen deposition and vascular endothelial growth factor mediated neovascularization in wound healing [57]. The most compelling evidence implicating IL-1β in pulmonary fibrosis comes from experiments involving transient overexpression of IL-1β induce tissue injury, subsequent local production of platelet-derived growth factor and TGF-β, and resultant pulmonary fibrosis [59].
Arachidonic acid metabolites
The study of arachidonic acid metabolites in fibrosis has significantly contributed to our understanding of the dichotomy between inflammation and fibrosis. COX-2 deficient mice are susceptible to pulmonary fibrosis [60]. Mice deficient in CC chemokine receptor 2 (CCR2), the receptor for monocyte chemottractant protein 1, were protected from induced pulmonary fibrosis but apparently not because of reduced inflammation. Alveolar epithelial cells from CCR2-deficient mice produce more PGE2, which has been associated with decreased fibrosis [61]. PGE2 inhibits the response of mesenchymal cells to profibrotic cytokines and is diminished in the lungs of patients with pulmonary fibrosis [62]. This has been linked to E prostanoid receptor loss following fibrotic lung injury. Lack of E prostanoid 2 expression is correlated with an inability of fibroblasts from bleomycin-treated mice to be inhibited by PGE2 [63]. Moreover, PGE2 and nitric oxide appear to function in parallel as autocrine/paracrine mediators of cytokine-driven fibroblast inhibition of the contraction of collagen gels and may contribute to remodelling during repair and inflammation [64]. Recent experiments have questioned the primary role of PGE2 in decreasing pulmonary fibrosis and implicated the ligand receptor pair prostacyclin and its receptor (IP) derived from ECs as the key mediator in limiting fibrosis in bleomycin lung injury models [16]. No change in response to bleomycin was noted in E prostanoid 2 and 4 receptor deficient mice. In stark contrast, IP deficiency limited both the development of the disease and consequential alterations in lung mechanics.
Transforming growth factor β
TGF-β plays a critical role in the fibroproliferative responses of the lung [65]. The TGF-β1 gene is upregulated in response to ALI [66]. The processes stimulated by TGF-β are critical to wound repair. TGF-β activation leads to reduction in cytokine production, promotes fibroblast recruitment, differentiation of myofibroblasts, and stimulation of extracellular matrix proteins. Animal studies have shown that expression levels of several TGF-β inducible genes are dramatically increased as early as 2 days after the induction of injury. In a model of ALI induced by nickel exposure, genes that decreased the most after nickel exposure were associated with fluid absorption, surfactant and phospholipid synthesis. Up-regulated genes included TGF-β inducible genes involved in the regulation of extracellular matrix function, fibroproliferation and fibrinolysis [9].
The significance of TGF-β in the regulation of the fibroproliferative phase of ARDS can be inferred from experimental data demonstrating that pharmacological inhibition of TGF-β protected wild-type mice from pulmonary oedema induced by bleomycin or Escherichia coli endotoxin [12]. In animal models, transfer of soluble TGF-β type II receptor ameliorates fibroproliferative changes in rat irradiated lungs [67]. In ARDS TGF-β expression may: (a) affect the gene expression of extracellular matrix molecules in stroma cells inducing collagen synthesis and inhibiting collagenase production [68]; (b) induce fibroproliferation [8], (c) establish an apparent state of autocrine stimulation in structural cells, including fibroblasts, resulting in chronic activation and possible differentiation to a more aggressive phenotype [69], and (d) promote the development of non-cardiogenic pulmonary oedema [12]. Resolution of pulmonary oedema is associated with improved clinical outcome [70] (the role of TGF-β in acute non-cardiogenic pulmonary oedema is further described in the accompanying contribution by Rocco and Pelosi).
Mechanisms of repair and remodelling
Stereotyped response to injury: pulmonary vs. extrapulmonary ALI
It remains unclear as to whether the fibroproliferative response to injury occurs in a stereotypical or an injury-specific manner. Evidence that this may be injury dependent comes from studies suggesting that pulmonary and extrapulmonary ARDS is pathologically different (see in the accompanying contribution by Negrini). Presumably after a direct insult the primary structure injured is the pulmonary epithelium. When the insult is extrapulmonary the main target for damage is the pulmonary endothelium [71, 72]. Figure 3 illustrates differences in matrix remodelling in pulmonary vs. extrapulmonary ARDS. Here primary ARDS is associated with a higher degree of pulmonary architectural distortion, cellular proliferation, collagen deposition and fragmentation of elastic bundles. These differences have not translated into differences in outcome, and no clear mechanistic explanations have been documented, but this may have significant implications for therapy.

Difference in matrix in pulmonary and extrapulmonary ARDS. a–i Morphological changes in early stages of diffuse alveolar damage from lungs of controls (normal and congestive heart failure patients), pulmonary and extrapulmonary ARDS patients. a Lungs from control show preserved architecture and thin alveolar septa. b Lung in primary pulmonary ARDS, characterized by architectural distortion and a homogeneous pattern of interstitial cell proliferation with hyaline membrane deposition along the internal surface of the alveolar wall (arrows). Alveolar spaces can be seen filled with exuberant plugs of fibrin. c Extrapulmonary ARDS, characterized almost exclusively by the presence of hyaline membrane lining alveolar walls and preserved pulmonary architecture. d–f Collagenous fibre staining from controls, pulmonary and extrapulmonary ARDS. Differences can be seen in collagen deposition between pulmonary and extrapulmonary ARDS. Lungs from the control groups and extrapulmonary ARDS (d, f) show preserved alveolar wall lining while in contrast patients with pulmonary ARDS (e) show dramatic distortion of the architecture and a diffuse picture of alveolar thickening associated with interstitial cell proliferation and hyaline membrane deposition. g–i Changes in alveolar elastic fibres. In lung samples from controls and extrapulmonary ARDS groups (g, i) the architecture of elastic components in the alveolus is maintained. h from lungs with primary pulmonary ARDS demonstrate sparse and fragmented bundles of elastic system fibres. a–c H&E × 100; d–f picrosirius × 100; g–i Weigert's Resorcin_Fuchin × 100 (reproduced with permission from [98])
A recent study has suggested that lung COX-2 gene expression is induced only by indirect mechanisms related to the systemic response to endotoxin rather than directly in response to inhaled endotoxin [73]. In contrast, release of the anti-inflammatory cytokine IL-10 is associated with a threefold increase in BAL fluid from animals exposed to an intrapulmonary source of ALI [74]. Moreover, given the same pulmonary mechanical dysfunction, independently of the cause of injury, an insult to the pulmonary epithelium has been proposed to lead to a more pronounced pro-inflammatory response than an injury to the endothelium [75]. Interestingly, however, the amount of collagen (matrix remodelling) may be similar in both pulmonary and extrapulmonary ALI, implying that inflammation and fibrosis are dissociated.
Resolution vs. fibrosis
Functional recovery from ARDS/ALI depends upon resolution of the underlying disorder: oedema clearance and resorption of the coagulum. Oedema clearance has been reviewed in detail [70]. Briefly, liquid is gradually cleared from airspaces by ion pumps that transport sodium with osmotically driven water movement across the alveolar epithelial membrane. Catecholamines may expedite fluid resorption, and delayed fluid clearance has been purported to impact negatively on resolution of ARDS/ALI. The following section reviews the repair, resorption and remodelling of the coagulum, focusing on the role of the coagulation cascade and rennin-angiotensin system.
Coagulation-fibrinolysis and the provisional membrane
The alveolar wall is an extremely delicate structure. The lung defends this precarious barrier from structural damage by expressing a high level of procoagulants. The alveolar proteinaceous exudate provides substrate for thrombin activation and fibrin formation. Local thrombin activation of activated protein C and complexing of thrombin to plasma-derived anti-thrombin III limits thrombin formation. Concurrently, low but significant levels of plasminogen activator urokinase (uPA) are continuously released along alveolar surfaces to facilitate resolution of extensive fibrin deposition on the basement membrane. Deficiency in urokinase and tissue plasminogen activators results in spontaneous appearance of fibrin and lung fibrosis in mice [76]. Mice with homozygous deletion of the plasminogen activator inhibitor 1 gene [PAI-1 (-/-)] are relatively protected from bleomycin-induced pulmonary fibrosis [77, 78]. Fibrosis is also reduced when plasminogen activation is enhanced in mice genetically engineered to express an inducible uPA transgene or after administration of uPA gene [79]. Conversely, fibrosis is worsened in mice having a constitutively active PAI-1 transgene or in mice that are genetically deficient in plasminogen [80]. Moreover, thrombin and factor Xa exert potent pro-fibrotic effects via proteolytic activation of the PAR-1 and the production of potent pro-fibrotic mediators [81]. PAR-1 expression also increased in response to lung injury and direct thrombin inhibition attenuates the fibrotic response to bleomycin in vivo [82]. Decreases in activated protein C levels are associated with increased collagen deposition in the lung [83].
The pulmonary endothelium is also actively involved in the fibrinolytic process, expressing plasminogen activators as well as their inhibitors. The EC fibrinolytic activity appears to be affected by several ARDS-related mediators including endotoxin, IL-1β, TNF-α and thrombin. Depression of fibrinolytic activity occurs as a result of inhibition of uPA by plasminogen activators, or series inhibition of plasmin by antiplasmins. Locally increased amplification of PAI-1 is largely responsible for this fibrinolytic defect [84]. The uPAR/PAI1 system has also been proposed to coordinate with integrins to regulate cell–cell matrix interactions [85].
Resorption and removal of the provisional membrane
In parallel with resorption of proteinaceous deposits is the removal of other matrix components. Imbalanced turnover of extracellular matrix is a hallmark of tissue injury. Persistent inflammation and fibroproliferation may result from failure to adequately remove extracellular matrix. Matrix metalloproteinases and their inhibitors (tissue inhibitors of metalloproteinases) play a key role in matrix degradation and turn over, and these have been extensively reviewed [86].
Recently the turnover of matrix hyaluronan has been implicated in the pathogenesis of ALI. In non-injured lungs this large glycosaminoglycan molecule exists in a high molecular weight conformation. Accumulation of low-molecular weight species occurs following tissue injury and inflammation. Clearance of hyaluronans from extracellular fluids occurs through macrophage scavenger receptors CD44. Recently Jiang et al. [87] found that Toll-like receptors 2 and 4—chief innate immune receptors in the response to Gram-negative and Gram-positive bacteria—may act in concert to either promote inflammation when bound to the low molecular weight form of hyaluronan or prevent apoptosis and attenuate lung injury when bound to the high molecular weight form of the molecule. In a bleomycin model of ALI, animals deficient in either Toll-like receptor 2 or 4 (double knock outs) or MyD88 developed increased interstitial thickening in lung tissues and protein accumulation in BAL fluid in response to injury, despite decreased neutrophil infiltration. Lung epithelial cell specific over expression of high molecular mass hyaluronan was found to be protective against ALI and alveolar epithelial cells apoptosis; in fact, over-expression of the enzyme responsible for the synthesis of the high-molecular weight form of this molecule results in decreased apoptosis. Moreover, blocking of binding to low-molecular hyaluronan resulted in decreased apoptosis, suggesting that signalling through the low molecular weight form of this molecule is pro-injurious [87]. This finding fits well with the current hypothesis that apoptosis early in the course of ALI is an important tissue survival mechanism where apoptosis prevents necrosis, thus preserving the scaffold for subsequent cell growth [22]. In addition, the synthesis of low molecular weight hyaluronan is dependent upon the activity of hyaluronan synthase 3 (Has3). Mice deficient in the latter are partially protected from injurious mechanical ventilation, suggesting a key role for this hyaluronan signalling pathways involving ventilator induced lung injury and matrix deposition and turnover [88].
The renin angiotensin system in lung remodelling
ANG II, generated by activation of local renin-angiotensin systems, has recently gained much attention as an important mediator in tissue repair and remodelling, in part via a TGF-β mediated mechanism. Angiotensin-converting enzyme (ACE) levels have been shown to be elevated in the BAL fluid and/or serum in many potentially fibrotic lung diseases including ARDS [89]. Mutations in this gene are associated with the development of and outcome from ARDS, suggesting a pathogenic role for the renin angiotensin system in ALI [90]. ACE inhibitors attenuate endothelial activation [91] and collagen deposition [92] during experimental lung injury, possibly via a reduction in epithelial cell apoptosis [93]. Moreover, ANG II could influence the progression of lung injury via a number of mechanisms. Evidence suggests that this protein acts as a pro-apoptotic factor for alveolar epithelial cells in vitro via the AT1 receptor [94]. ANG II is mitogenic for human lung fibroblasts via activation of the AT1 receptor [95], implicating ANG II in the fibroproliferative response to lung injury. In vascular smooth muscle cells the cellular actions of ANG II have been linked to the autocrine release of growth factors, such as platelet-derived growth factor, fibroblast growth factor, and TGF-β [96].
More recently Marshall and colleagues [95] have unambiguously implicated ANG II in the fibroproliferative response to lung injury. In vitro ANG II is a potent stimulator of lung fibroblast collagen production via the AT1 receptor, and this appears to be in part mediated by TGF-β. After bleomycin-induced lung injury increased ANG II concentrations preceded a doubling of lung collagen. While lung ACE activity remained unchanged, administration of an ACE inhibitor attenuated lung ACE activity, ANG II concentrations and collagen deposition. Treatment with an AT1 receptor antagonist also reduced lung collagen deposition and increased ANG II levels. Together these data support the hypothesis that ANG II, possibly generated within the lung during acute injury, contributes directly to lung collagen deposition via fibroblast activation. However, the efficacy of ACE inhibition in this model may also involve actions unrelated to ANG II generation [97].
Conclusions
Factors and circumstances that determine whether areas of the lung heal with minimal injury or progress to irreversible fibrosis need to be defined and may indeed lead to the development of novel therapeutic approaches to the management of ARDS. Traditionally, processes of repair and remodelling were thought of as late events in the course of ARDS. A key point highlighted in this review is that fibroproliferation in ARDS does not occur in sequence, or in parallel with inflammation, but is the summation of various intertwined processes that likely begin immediately after the onset of injury and may be injury specific. Moreover, this is not only affected by an internal hierarchy of interactions but is modulated by genetic and environmental factors, thus setting the stage for potential early chemotherapeutic modulation in the future.
References
Meduri GU (1996) The role of the host defence response in the progression and outcome of ARDS: pathophysiological correlations and response to glucocorticoid treatment. Eur Respir J 9:2650–2670
Andrews P, Azoulay E, Antonelli M, Brochard L, Brun-Buisson C, De Backer D, Dobb G, Fagon JY, Gerlach H, Groeneveld J, Macrae D, Mancebo J, Metnitz P, Nava S, Pugin J, Pinsky M, Radermacher P, Richard C (2007) Year in review in Intensive Care Medicine, 2006. II. Infections and sepsis, haemodynamics, elderly, invasive and noninvasive mechanical ventilation, weaning, ARDS. Intensive Care Med 33:214–229
Marshall R, Bellingan G, Laurent G (1998) The acute respiratory distress syndrome: fibrosis in the fast lane. Thorax 53:815–817
Bellingan GJ (2002) The pulmonary physician in critical care *6: the pathogenesis of ALI/ARDS. Thorax 57:540–546
Geiser T (2003) Mechanisms of alveolar epithelial repair in acute lung injury-a translational approach. Swiss Med Wkly 133:586–590
Chapman HA (2004) Disorders of lung matrix remodeling. J Clin Invest 113:148–157
Chesnutt AN, Matthay MA, Tibayan FA, Clark JG (1997) Early detection of type III procollagen peptide in acute lung injury. Pathogenetic and prognostic significance. Am J Respir Crit Care Med 156:840–845
Marshall RP, Bellingan G, Webb S, Puddicombe A, Goldsack N, McAnulty RJ, Laurent GJ (2000) Fibroproliferation occurs early in the acute respiratory distress syndrome and impacts on outcome. Am J Respir Crit Care Med 162:1783–1788
Wesselkamper SC, Case LM, Henning LN, Borchers MT, Tichelaar JW, Mason JM, Dragin N, Medvedovic M, Sartor MA, Tomlinson CR, Leikauf GD (2005) Gene expression changes during the development of acute lung injury: role of transforming growth factor beta. Am J Respir Crit Care Med 172:1399–1411
Weinberger SE, Kelman JA, Elson NA, Young RC Jr, Reynolds HY, Fulmer JD, Crystal RG (1978) Bronchoalveolar lavage in interstitial lung disease. Ann Intern Med 89:459–466
Keogh BA, Crystal RG (1982) Alveolitis: the key to the interstitial lung disorders. Thorax 37:1–10
Pittet JF, Griffiths MJ, Geiser T, Kaminski N, Dalton SL, Huang X, Brown LA, Gotwals PJ, Koteliansky VE, Matthay MA, Sheppard D (2001) TGF-beta is a critical mediator of acute lung injury. J Clin Invest 107:1537–1544
Ichikado K, Suga M, Muranaka H, Gushima Y, Miyakawa H, Tsubamoto M, Johkoh T, Hirata N, Yoshinaga T, Kinoshita Y, Yamashita Y, Sasaki Y (2006) Prediction of prognosis for acute respiratory distress syndrome with thin-section CT: validation in 44 cases. Radiology 238:321–329
Meduri GU (1993) Late adult respiratory distress syndrome. New Horiz 1:563–577
Munger JS, Huang X, Kawakatsu H, Griffiths MJ, Dalton SL, Wu J, Pittet JF, Kaminski N, Garat C, Matthay MA, Rifkin DB, Sheppard D (1999) The integrin alpha v beta 6 binds and activates latent TGF beta 1: a mechanism for regulating pulmonary inflammation and fibrosis. Cell 96:319–328
Lovgren AK, Jania LA, Hartney JM, Parsons KK, Audoly LP, Fitzgerald GA, Tilley SL, Koller BH (2006) COX-2-derived Prostacyclin Protects Against Bleomycin-induced Pulmonary Fibrosis. Am J Physiol Lung Cell Mol Physiol 291:L144–156
Kuwano K, Hagimoto N, Nakanishi Y (2004) The role of apoptosis in pulmonary fibrosis. Histol Histopathol 19:867–881
Tamby MC, Chanseaud Y, Humbert M, Fermanian J, Guilpain P, Garcia-de-la-Pena-Lefebvre, Brunet S, Servettaz A, Weill B, Simonneau G, Guillevin L, Boissier MC, Mouthon L (2005) Anti-endothelial cell antibodies in idiopathic and systemic sclerosis associated pulmonary arterial hypertension. Thorax 60:765–772
Horowitz JC, Cui Z, Moore TA, Meier TR, Reddy RC, Toews GB, Standiford TJ, Thannickal VJ (2006) Constitutive activation of prosurvival signaling in alveolar mesenchymal cells isolated from patients with nonresolving acute respiratory distress syndrome. Am J Physiol Lung Cell Mol Physiol 290:L415–L425
Warburton D, Tefft D, Mailleux A, Bellusci S, Thiery JP, Zhao J, Buckley S, Shi W, Driscoll B (2001) Do lung remodeling, repair, and regeneration recapitulate respiratory ontogeny? Am J Respir Crit Care Med 164:S59–S62
Watkins DN, Berman DM, Burkholder SG, Wang B, Beachy PA, Baylin SB (2003) Hedgehog signalling within airway epithelial progenitors and in small-cell lung cancer. Nature 422:313–317
Douglas IS, Diaz DV, Winn RA, Voelkel NF (2006) Beta-catenin in the fibroproliferative response to acute lung injury. Am J Respir Cell Mol Biol 34:274–285
Hong KU, Reynolds SD, Watkins S, Fuchs E, Stripp BR (2004) Basal cells are a multipotent progenitor capable of renewing the bronchial epithelium. Am J Pathol 164:577–588
Borthwick DW, Shahbazian M, Krantz QT, Dorin JR, Randell SH (2001) Evidence for stem-cell niches in the tracheal epithelium. Am J Respir Cell Mol Biol 24:662–670
Porter RM, Lane EB (2003) Phenotypes, genotypes and their contribution to understanding keratin function. Trends Genet 19:278–285
Kotton DN, Ma BY, Cardoso WV, Sanderson EA, Summer RS, Williams MC, Fine A (2001) Bone marrow-derived cells as progenitors of lung alveolar epithelium. Development 128:5181–5188
Yamada M, Kubo H, Kobayashi S, Ishizawa K, Numasaki M, Ueda S, Suzuki T, Sasaki H (2004) Bone marrow-derived progenitor cells are important for lung repair after lipopolysaccharide-induced lung injury. J Immunol 172:1266–1272
Rojas M, Xu J, Woods CR, Mora AL, Spears W, Roman J, Brigham KL (2005) Bone marrow-derived mesenchymal stem cells in repair of the injured lung. Am J Respir Cell Mol Biol 33:145–152
Gomperts BN, Belperio JA, Rao PN, Randell SH, Fishbein MC, Burdick MD, Strieter RM (2006) Circulating progenitor epithelial cells traffic via CXCR4/CXCL12 in response to airway injury. J Immunol 176:1916–1927
Uhal BD (2002) Apoptosis in lung fibrosis and repair. Chest 122:293S–298S
Li HP, Li X, He GJ, Yi XH, Kaplan AP (2004) The influence of dexamethasone on the proliferation and apoptosis of pulmonary inflammatory cells in bleomycin-induced pulmonary fibrosis in rats. Respirology 9:25–32
Kuwano K, Hagimoto N, Hara N (2001) Molecular mechanisms of pulmonary fibrosis and current treatment. Curr Mol Med 1:551–573
Wang HC, Shun CT, Hsu SM, Kuo SH, Luh KT, Yang PC (2002) Fas/Fas ligand pathway is involved in the resolution of type II pneumocyte hyperplasia after acute lung injury: evidence from a rat model. Crit Care Med 30:1528–1534
Budinger GR, Chandel NS (2001) The role of cell suicide or apoptosis in the pathophysiology of acute lung injury. Intensive Care Med 27:1091–1093
Wang R, Zagariya A, Ang E, Ibarra-Sunga O, Uhal BD (1999) Fas-induced apoptosis of alveolar epithelial cells requires ANG II generation and receptor interaction. Am J Physiol 277:L1245–L1250
Hagimoto N, Kuwano K, Inoshima I, Yoshimi M, Nakamura N, Fujita M, Maeyama T, Hara N (2002) TGF-beta 1 as an enhancer of Fas-mediated apoptosis of lung epithelial cells. J Immunol 168:6470–6478
Sookhai S, Wang JJ, McCourt M, Kirwan W, Bouchier-Hayes D, Redmond P (2002) A novel therapeutic strategy for attenuating neutrophil-mediated lung injury in vivo. Ann Surg 235:285–291
Matute-Bello G, Lee JS, Liles WC, Frevert CW, Mongovin S, Wong V, Ballman K, Sutlief S, Martin TR (2005) Fas-mediated acute lung injury requires fas expression on nonmyeloid cells of the lung. J Immunol 175:4069–4075
Braude S, Apperley J, Krausz T, Goldman JM, Royston D (1985) Adult respiratory distress syndrome after allogeneic bone-marrow transplantation: evidence for a neutrophil-independent mechanism. Lancet 1:1239–1242
Winn R, Maunder R, Chi E, Harlan J (1987) Neutrophil depletion does not prevent lung edema after endotoxin infusion in goats. J Appl Physiol 62:116–121
Clark JG, Kuhn C 3rd (1982) Bleomycin-induced pulmonary fibrosis in hamsters: effect of neutrophil depletion on lung collagen synthesis. Am Rev Respir Dis 126:737–739
Aarbiou J, Ertmann M, van Wetering S, van Noort P, Rook D, Rabe KF, Litvinov SV, van Krieken JH, de Boer WI, Hiemstra PS (2002) Human neutrophil defensins induce lung epithelial cell proliferation in vitro. J Leukoc Biol 72:167–174
Aarbiou J, Verhoosel RM, van Wetering S, de Boer WI, van Krieken JH, Litvinov SV, Rabe KF, Hiemstra PS (2004) Neutrophil defensins enhance lung epithelial wound closure and mucin gene expression in vitro. Am J Respir Cell Mol Biol 30:193–201
MacGregor IR, Perrie AM, Donnelly SC, Haslett C (1997) Modulation of human endothelial thrombomodulin by neutrophils and their release products. Am J Respir Crit Care Med 155:47–52
Shih JY, Yang SC, Yu CJ, Wu HD, Liaw YS, Wu R, Yang PC (1997) Elevated serum levels of mucin-associated antigen in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med 156:1453–1457
Rose MC, Voynow JA (2006) Respiratory tract mucin genes and mucin glycoproteins in health and disease. Physiol Rev 86:245–278
Reynolds HY (2005) Lung inflammation and fibrosis: an alveolar macrophage-centered perspective from the 1970s to 1980s. Am J Respir Crit Care Med 171:98–102
Shimabukuro DW, Sawa T, Gropper MA (2003) Injury and repair in lung and airways. Crit Care Med 31:S524–S531
Dos Santos CC, Slutsky AS (2006) The contribution of biophysical lung injury to the development of biotrauma. Annu Rev Physiol 68:585–618
Beck-Schimmer B, Schwendener R, Pasch T, Reyes L, Booy C, Schimmer RC (2005) Alveolar macrophages regulate neutrophil recruitment in endotoxin-induced lung injury. Respir Res 6:61
Elder A, Johnston C, Gelein R, Finkelstein J, Wang Z, Notter R, Oberdorster G (2005) Lung inflammation induced by endotoxin is enhanced in rats depleted of alveolar macrophages with aerosolized clodronate. Exp Lung Res 31:527–546
Warner AE (1996) Pulmonary intravascular macrophages. Role in acute lung injury. Clin Chest Med 17:125–135
O'Dea KP, Young AJ, Yamamoto H, Robotham JL, Brennan FM, Takata M (2005) Lung-marginated monocytes modulate pulmonary microvascular injury during early endotoxemia. Am J Respir Crit Care Med 172:1119–1127
Olman MA, White KE, Ware LB, Simmons WL, Benveniste EN, Zhu S, Pugin J, Matthay MA (2004) Pulmonary edema fluid from patients with early lung injury stimulates fibroblast proliferation through IL-1 beta-induced IL-6 expression. J Immunol 172:2668–2677
Dayer JM, de Rochemonteix B, Burrus B, Demczuk S, Dinarello CA (1986) Human recombinant interleukin 1 stimulates collagenase and prostaglandin E2 production by human synovial cells. J Clin Invest 77:645–648
Portnoy J, Pan T, Dinarello CA, Shannon JM, Westcott JY, Zhang L, Mason RJ (2006) Alveolar type II cells inhibit fibroblast proliferation: role of IL-1alpha. Am J Physiol Lung Cell Mol Physiol 290:L307–L316
Ishida Y, Kondo T, Kimura A, Matsushima K, Mukaida N (2006) Absence of IL-1 Receptor Antagonist Impaired Wound Healing along with Aberrant NF-{kappa}B Activation and a Reciprocal Suppression of TGF-beta Signal Pathway. J Immunol 176:5598–5606
Belperio JA, DiGiovine B, Keane MP, Burdick MD, Ying XY, Ross DJ, Lynch JP 3rd, Kunkel SL, Strieter RM (2002) Interleukin-1 receptor antagonist as a biomarker for bronchiolitis obliterans syndrome in lung transplant recipients. Transplantation 73:591–599
Kolb M, Margetts PJ, Anthony DC, Pitossi F, Gauldie J (2001) Transient expression of IL-1beta induces acute lung injury and chronic repair leading to pulmonary fibrosis. J Clin Invest 107:1529–1536
Bonner JC, Rice AB, Ingram JL, Moomaw CR, Nyska A, Bradbury A, Sessoms AR, Chulada PC, Morgan DL, Zeldin DC, Langenbach R (2002) Susceptibility of cyclooxygenase-2-deficient mice to pulmonary fibrogenesis. Am J Pathol 161:459–470
Moore BB, Peters-Golden M, Christensen PJ, Lama V, Kuziel WA, Paine R 3rd, Toews GB (2003) Alveolar epithelial cell inhibition of fibroblast proliferation is regulated by MCP-1/CCR2 and mediated by PGE2. Am J Physiol Lung Cell Mol Physiol 284:L342–L349
Wilborn J, Crofford LJ, Burdick MD, Kunkel SL, Strieter RM, Peters-Golden M (1995) Cultured lung fibroblasts isolated from patients with idiopathic pulmonary fibrosis have a diminished capacity to synthesize prostaglandin E2 and to express cyclooxygenase-2. J Clin Invest 95:1861–1868
Moore BB, Ballinger MN, White ES, Green ME, Herrygers AB, Wilke CA, Toews GB, Peters-Golden M (2005) Bleomycin-induced E prostanoid receptor changes alter fibroblast responses to prostaglandin E2. J Immunol 174:5644–5649
Zhu YK, Liu XD, Skold MC, Umino T, Wang H, Romberger DJ, Spurzem JR, Kohyama T, Wen FQ, Rennard SI (2001) Cytokine inhibition of fibroblast-induced gel contraction is mediated by PGE (2) and NO acting through separate parallel pathways. Am J Respir Cell Mol Biol 25:245–253
Bartram U, Speer CP (2004) The role of transforming growth factor beta in lung development and disease. Chest 125:754–765
Fahy RJ, Lichtenberger F, McKeegan CB, Nuovo GJ, Marsh CB, Wewers MD (2003) The acute respiratory distress syndrome: a role for transforming growth factor-beta 1. Am J Respir Cell Mol Biol 28:499–503
Nishioka A, Ogawa Y, Mima T, Jin YJ, Sonobe H, Kariya S, Kubota K, Yoshida S, Ueno H (2004) Histopathologic amelioration of fibroproliferative change in rat irradiated lung using soluble transforming growth factor-beta (TGF-beta) receptor mediated by adenoviral vector. Int J Radiat Oncol Biol Phys 58:1235–1241
Kaminski N, Allard JD, Pittet JF, Zuo F, Griffiths MJ, Morris D, Huang X, Sheppard D, Heller RA (2000) Global analysis of gene expression in pulmonary fibrosis reveals distinct programs regulating lung inflammation and fibrosis. Proc Natl Acad Sci USA 97:1778–1783
Dhainaut JF, Charpentier J, Chiche JD (2003) Transforming growth factor-beta: a mediator of cell regulation in acute respiratory distress syndrome. Crit Care Med 31:S258–S264
Matthay MA, Robriquet L, Fang X (2005) Alveolar epithelium: role in lung fluid balance and acute lung injury. Proc Am Thorac Soc 2:206–213
Gattinoni L, Pelosi P, Suter PM, Pedoto A, Vercesi P, Lissoni A (1998) Acute respiratory distress syndrome caused by pulmonary and extrapulmonary disease. Different syndromes? Am J Respir Crit Care Med 158:3–11
Zimmerman GA, Albertine KH, Carveth HJ, Gill EA, Grissom CK, Hoidal JR, Imaizumi T, Maloney CG, McIntyre TM, Michael JR, Orme JF, Prescott SM, Topham MS (1999) Endothelial activation in ARDS. Chest 116:18S–24S
Sadikot RT, Jansen ED, Blackwell TR, Zoia O, Yull F, Christman JW, Blackwell TS (2001) High-dose dexamethasone accentuates nuclear factor-kappa b activation in endotoxin-treated mice. Am J Respir Crit Care Med 164:873–878
Menezes SL, Bozza PT, Neto HC, Laranjeira AP, Negri EM, Capelozzi VL, Zin WA, Rocco PR (2005) Pulmonary and extrapulmonary acute lung injury: inflammatory and ultrastructural analyses. J Appl Physiol 98:1777–1783
Santos FB, Nagato LK, Boechem NM, Negri EM, Guimaraes A, Capelozzi VL, Faffe DS, Zin WA, Rocco PR (2006) Time course of lung parenchyma remodeling in pulmonary and extrapulmonary acute lung injury. J Appl Physiol 100:98–106
Carmeliet P, Schoonjans L, Kieckens L, Ream B, Degen J, Bronson R, De Vos R, van den Oord JJ, Collen D, Mulligan RC (1994) Physiological consequences of loss of plasminogen activator gene function in mice. Nature 368:419–424
Eitzman DT, McCoy RD, Zheng X, Fay WP, Shen T, Ginsburg D, Simon RH (1996) Bleomycin-induced pulmonary fibrosis in transgenic mice that either lack or overexpress the murine plasminogen activator inhibitor-1 gene. J Clin Invest 97:232–237
Hattori N, Degen JL, Sisson TH, Liu H, Moore BB, Pandrangi RG, Simon RH, Drew AF (2000) Bleomycin-induced pulmonary fibrosis in fibrinogen-null mice. J Clin Invest 106:1341–1350
Sisson TH, Hanson KE, Subbotina N, Patwardhan A, Hattori N, Simon RH (2002) Inducible lung-specific urokinase expression reduces fibrosis and mortality after lung injury in mice. Am J Physiol Lung Cell Mol Physiol 283:L1023–L1032
Swaisgood CM, French EL, Noga C, Simon RH, Ploplis VA (2000) The development of bleomycin-induced pulmonary fibrosis in mice deficient for components of the fibrinolytic system. Am J Pathol 157:177–187
Blanc-Brude OP, Archer F, Leoni P, Derian C, Bolsover S, Laurent GJ, Chambers RC (2005) Factor Xa stimulates fibroblast procollagen production, proliferation, and calcium signaling via PAR1 activation. Exp Cell Res 304:16–27
Howell DC, Goldsack NR, Marshall RP, McAnulty RJ, Starke R, Purdy G, Laurent GJ, Chambers RC (2001) Direct thrombin inhibition reduces lung collagen, accumulation, and connective tissue growth factor mRNA levels in bleomycin-induced pulmonary fibrosis. Am J Pathol 159:1383–1395
Suzuki K, Gabazza EC, Hayashi T, Kamada H, Adachi Y, Taguchi O (2004) Protective role of activated protein C in lung and airway remodeling. Crit Care Med 32:S262–S265
Jesmin S, Gando S, Matsuda N, Sakuma I, Kobayashi S, Sakuraya F, Hattori Y (2004) Temporal changes in pulmonary expression of key procoagulant molecules in rabbits with endotoxin-induced acute lung injury: elevated expression levels of protease-activated receptors. Thromb Haemost 92:966–979
Wei Y, Eble JA, Wang Z, Kreidberg JA, Chapman HA (2001) Urokinase receptors promote beta1 integrin function through interactions with integrin alpha3beta1. Mol Biol Cell 12:2975–2986
Parks WC (2003) Matrix metalloproteinases in lung repair. Eur Respir J Suppl 44:36s–38s
Jiang D, Liang J, Fan J, Yu S, Chen S, Luo Y, Prestwich GD, Mascarenhas MM, Garg HG, Quinn DA, Homer RJ, Goldstein DR, Bucala R, Lee PJ, Medzhitov R, Noble PW (2005) Regulation of lung injury and repair by Toll-like receptors and hyaluronan. Nat Med 11:1173–1179
Bai KJ, Spicer AP, Mascarenhas MM, Yu L, Ochoa CD, Garg HG, Quinn DA (2005) The role of hyaluronan synthase 3 in ventilator-induced lung injury. Am J Respir Crit Care Med 172:92–98
Fourrier F, Chopin C, Wallaert B, Mazurier C, Mangalaboyi J, Durocher A (1985) Compared evolution of plasma fibronectin and angiotensin-converting enzyme levels in septic ARDS. Chest 87:191–195
Marshall RP, Webb S, Bellingan GJ, Montgomery HE, Chaudhari B, McAnulty RJ, Humphries SE, Hill MR, Laurent GJ (2002) Angiotensin converting enzyme insertion/deletion polymorphism is associated with susceptibility and outcome in acute respiratory distress syndrome. Am J Respir Crit Care Med 166:646–650
Ward WF, Molteni A, Ts'ao CH, Hinz JM (1990) Captopril reduces collagen and mast cell accumulation in irradiated rat lung. Int J Radiat Oncol Biol Phys 19:1405–1409
Wang R, Ibarra-Sunga O, Verlinski L, Pick R, Uhal BD (2000) Abrogation of bleomycin-induced epithelial apoptosis and lung fibrosis by captopril or by a caspase inhibitor. Am J Physiol Lung Cell Mol Physiol 279:L143–L151
Ward WF, Molteni A, Ts'ao CH, Kim YT, Hinz JM (1992) Radiation pneumotoxicity in rats: modification by inhibitors of angiotensin converting enzyme. Int J Radiat Oncol Biol Phys 22:623–625
Wang R, Zagariya A, Ibarra-Sunga O, Gidea C, Ang E, Deshmukh S, Chaudhary G, Baraboutis J, Filippatos G, Uhal BD (1999) Angiotensin II induces apoptosis in human and rat alveolar epithelial cells. Am J Physiol 276:L885–L889
Marshall RP, McAnulty RJ, Laurent GJ (2000) Angiotensin II is mitogenic for human lung fibroblasts via activation of the type 1 receptor. Am J Respir Crit Care Med 161:1999–2004
Weber H, Taylor DS, Molloy CJ (1994) Angiotensin II induces delayed mitogenesis and cellular proliferation in rat aortic smooth muscle cells. Correlation with the expression of specific endogenous growth factors and reversal by suramin. J Clin Invest 93:788–798
Marshall RP, Gohlke P, Chambers RC, Howell DC, Bottoms SE, Unger T, McAnulty RJ, Laurent GJ (2004) Angiotensin II and the fibroproliferative response to acute lung injury. Am J Physiol Lung Cell Mol Physiol 286:L156–L164
Negri EM, Hoelz C, Barbas CS, Montes GS, Saldiva PH, Capelozzi VL (2002) Acute remodeling of parenchyma in pulmonary and extrapulmonary ARDS. An autopsy study of collagen-elastic system fibers. Pathol Res Pract 198:355–361
Acknowledgements
This work was supported by the Parker B. Francis Foundation.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is discussed in the editorial available at: http://dx.doi.org/10.1007/s00134-007-0965-8.
Rights and permissions
About this article
Cite this article
Dos Santos, C.C. Advances in mechanisms of repair and remodelling in acute lung injury. Intensive Care Med 34, 619–630 (2008). https://doi.org/10.1007/s00134-007-0963-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-007-0963-x