
Abstract
Objective
To monitor the use of drotrecogin alfa activated (DrotAA) in Italy and its effects on patients' health.
Design
Prospective pharmaco-surveillance program with a parallel non-randomized control group.
Setting
The Ministry of Health required all intensive care units (ICUs) using DrotAA to participate in the pharmaco-surveillance program. Our control group was formed of patients eligible for treatment with DrotAA but who had not received it.
Patients and participants
The data we collected included basic demographic characteristics, indications, modalities of use, adverse events, and ICU mortality. We identified potentially non-collaborating centres on the basis of data on DrotAA purchasing by hospitals.
Measurements and results
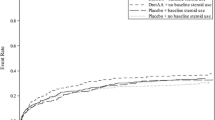
From 2003 to 2006, 668 cases of treatment with DrotAA were reported. We estimate that 79.3% of all patients treated in Italy in this period were recruited. Off-label use was common. Delayed start was the main reason for off-label prescription. Bleeding during infusion occurred in 73 patients (10.9%). The ICU mortality was higher in patients with bleeding (57.5 vs. 44.9%; p = 0.041). Crude ICU mortality was lower in patients receiving DrotAA than in controls (46.4 vs. 54.9%; p = 0.0004); however, multivariate analysis, which adjusted for certain relevant differences, showed that DrotAA treatment was associated with higher mortality after scheduled surgery.
Conclusions
These results question the way in which the drug is used in everyday clinical practice and its efficacy in a selected subgroup, and reinforce the need for a new, independent, confirmatory trial to reassess the risk-to-benefit ratio of DrotAA.


Similar content being viewed by others


References
Alberti C, Brun-Buisson C, Burchardi H, Martin C, Goodman S, Artigas A, Sicignano A, Palazzo M, Moreno R, Boulme R, Lepage E, Le Gall R (2002) Epidemiology of sepsis and infection in ICU patients from an international multicentre cohort study. Intensive Care Med 28:108–121
Linde-Zwirble WT, Angus DC (2004) Severe sepsis epidemiology: sampling, selection, and society. Crit Care 8:222–226
Bernard GR, Vincent JL, Laterre PF, LaRosa SP, Dhainaut JF, Lopez-Rodriguez A, Steingrub JS, Garber GE, Helterbrand JD, Ely EW, Fisher CJ Jr (2001) Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med 344:699–709
EMEA. European Public Assessment Report. Scientific discussion for the approval of Xigris. Accessed in January 2006 at: http://www.emea.eu.int/humandocs/Humans/EPAR/xigris/Xigris.htm
EMEA. Guideline on procedures for the granting of a marketing authorisation under exceptional circumstances, pursuant to article 14 (8) of regulation (ec) no 726/2004. Accessed in January 2006 at: http://www.emea.eu.int/pdfs/human/euleg/35798105en.pdf
Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM, Vincent JL, Ramsay G (2003) 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Med 29:530–538
Le Gall JR, Lemeshow S, Saulnier F (1993) A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. J Am Med Assoc 270:2957–2963
Vincent JL, Mendonca A de, Cantraine F, Moreno R, Takala J, Suter PM, Sprung CL, Colardyn F, Blecher S (1998) Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit Care Med 26:1793–1800
Boffelli S, Rossi C, Anghileri A, Giardino M, Carnevale L, Messina M, Neri M, Langer M, Bertolini G (2006) Continuous quality improvement in Intensive Care Medicine. The GiViTI Margherita Project: Report 2005. Minerva Anestesiol 72:419–432
Garner J, Jarvis W, Emori T, Horan T, Hughes J (1996) CDC definitions for nosocomial infections. In: Olmsted R (ed) APIC infection control and applied epidemiology: principles and practice. Mosby, St. Louis, pp A1–A20
Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, Schein RM, Sibbald WJ (1992) Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest 101:1644–1655
EMEA. Xigris: Product information. Accessed in November 2006 at: http://www.emea.eu.int/humandocs/PDFs/EPAR/xigris/H-396-PI-en.pdf
Hosmer D, Lemeshow S (1989) Applied logistic regression. Wiley, New York
Dhainaut JF, Laterre PF, Janes JM, Bernard GR, Artigas A, Bakker J, Riess H, Basson BR, Charpentier J, Utterback BG, Vincent JL (2003) Drotrecogin alfa (activated) in the treatment of severe sepsis patients with multiple-organ dysfunction: data from the PROWESS trial. Intensive Care Med 29:894–903
Abraham E, Laterre PF, Garg R, Levy H, Talwar D, Trzaskoma BL, Francois B, Guy JS, Bruckmann M, Rea-Neto A, Rossaint R, Perrotin D, Sablotzki A, Arkins N, Utterback BG, Macias WL (2005) Drotrecogin alfa (activated) for adults with severe sepsis and a low risk of death. N Engl J Med 353:1332–1341
Mackenzie AF (2005) Activated protein C: Do more survive? Intensive Care Med 31:1624–1626
Carlet J (2006) Prescribing indications based on successful clinical trials in sepsis: a difficult exercise. Crit Care Med 34:525–529
Eichacker PQ, Danner RL, Suffredini AF, Cui X, Natanson C (2005) Reassessing recombinant human activated protein C for sepsis: time for a new randomized controlled trial. Crit Care Med 33:2426–2428
Hazell L, Shakir SAW (2006) Under-reporting of adverse drug reactions: a systematic review. Drug Safety 29:385–396
Vincent JL, Bernard GR, Beale R, Doig C, Putensen C, Dhainaut JF, Artigas A, Fumagalli R, Macias W, Wright T, Wong K, Sundin DP, Turlo MA, Janes J (2005) Drotrecogin alfa (activated) treatment in severe sepsis from the global open-label trial ENHANCE: further evidence for survival and safety and implications for early treatment. Crit Care Med 33:2266–2277
Steingrub J, Sanchez P, Zeckel M, Bates B, Qualy R (2003) Safety of drotrecogin alfa (activated): results of MERCURY, a retrospective multicenter observational study. Crit Care Med 31 (12 Suppl):A117
Cohen J, Guyatt G, Bernard GR, Calandra T, Cook D, Elbourne D, Marshall J, Nunn A, Opal S (2001) New strategies for clinical trials in patients with sepsis and septic shock. Crit Care Med 29:880–886
Acknowledgements
This study was funded by the Italian Medicines Agency of the Ministry of Health (AIFA – “Agenzia Italiana del Farmaco”) and carried out in collaboration with AIFA and the “Gruppo Italiano per la Valutazione degli Interventi in Terapia Intensiva” (GiViTI). GiViTI is the recipient of unconditioned grants from AstraZeneca Italy, Sanofi-Aventis Italy and Draeger Italia, none of which were involved in this study in any way. The authors substantially contributed to: conception and design (G. B., S. L., A. Ad., D. P.), analysis (G. B., C. R.) and interpretation (all authors) of data, the drafting (G. B., D. P.) or critical revision (C. R., S. L., A. Ad., A. Am.) of the article. All of them approved the final version of the manuscript. The full list of participating centres is given in the online supplement. G. Bertolini had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. GiViTI Steering Committee: N. Latronico, Brescia; M. Tavola, Lecco; D. Radrizzani, Legnano (MI); D. Giudici, M. Langer, A. Sicignano, Milan; M. Messina, Olbia; R. Tetamo, Palermo; P. Malacarne, Pisa; G. Bertolini, Ranica (BG); G. Nardi, Rome; S. Livigni, Torino; E. Nascimben, Treviso.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is discussed in the editorial available at: http://dx.doi.org/10.1007/s00134-007-0556-8
Electronic supplementary material
Rights and permissions
About this article
Cite this article
Bertolini, G., Rossi, C., Anghileri, A. et al. Use of Drotrecogin alfa (activated) in Italian intensive care units: the results of a nationwide survey. Intensive Care Med 33, 426–434 (2007). https://doi.org/10.1007/s00134-007-0554-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-007-0554-x