
Abstract
Objective
To demonstrate the diagnostic yield, therapeutic role and safety of flexible bronchoscopy via an intensivist-led service in critically ill children.
Design
Retrospective chart review.
Setting
Regional paediatric intensive care unit.
Measurements and results
One hundred forty-eight flexible bronchoscopies were performed by two intensivists on 134 patients (median age 16.5 months) over a 2.5-year period. Eighty-eight percent of patients required mechanical ventilation, and 22% were receiving inotropes. Case mix included general (n = 77), cardiac surgery (n = 18), cardiology (n = 13), ear-nose-and-throat surgery (n = 17), oncology (n = 8) and renal (n = 1). The indication for bronchoscopy was defined a priori according to one of four categories: suspected upper airway disease (n = 32); lower airway disease (n = 70); investigation of pulmonary disease (n = 25); and extubation failure (n = 21). Bronchoscopy was generally performed soon after PICU admission, at a median time of 1.5 days for the former three categories, and 4 days for extubation failure group. A positive yield from bronchoscopy (diagnosis that explained the clinical condition or influenced patient management) was present in 113 of 148 (76%) procedures, varying within groups from 44% (pulmonary disease) to 90% (extubation failure).Ten percent of patients developed a fall in oxygen saturations > 20% during the procedure and 17% required a bolus of at least 10 ml/kg of 0.9% saline for hypotension.
Conclusions
Critically ill patients with respiratory problems may benefit from a PICU-led bronchoscopy service as the yield for positive bronchoscopic finding is high, particularly for upper airway problems or extubation failure.
Similar content being viewed by others



Introduction
Flexible bronchoscopy using modern ultra-thin fibreoptic technology has revolutionised the investigation of neonatal and paediatric airway disorders over the past two decades [1, 2, 3, 4, 5, 6, 7, 8]. Traditionally flexible bronchoscopy has been performed by pulmonologists. This is reflected in the majority of reports to date, where bronchoscopic indications have been largely diagnostic, and typically performed on stable, self-ventilating patients [2, 3, 4, 5, 6, 7, 8].
Flexible bronchoscopy is now used increasingly in critically ill patients, resulting in a wider range of therapeutic applications, e.g. removal of mucus plugs in acute lobar atelectasis, and treatment of plastic bronchitis in the acute chest syndrome [2, 9, 10, 11, 12]. Bronchoscopy in this setting can also carry greater risk, as critically ill children may have severe gas exchange abnormalities, haemodynamic instability or significant co-morbidity such as congenital heart disease or pulmonary hypertension.
We established an in-house, intensivist-led flexible bronchoscopy service in our 20-bed multidisciplinary paediatric intensive care unit (PICU) in 2002. This facility was set up to augment a pre-existing ear-nose-and-throat (ENT) surgical service, and also with the aim of providing early access to bronchoscopy for non-ENT PICU patients. Our goals were twofold: to maximise the diagnostic and therapeutic potential from flexible bronchoscopy while minimising the complication rate; however, on review of the literature at the time, it was unclear as to which patients would most likely benefit from flexible bronchoscopy, and what the complication rate was liable to be in our patient cohort. This was for a variety of reasons: (a) the majority of procedures reported in the literature were on non-ventilated children (the mechanical ventilation rate in our unit is typically 80%); (b) many of the patients in the literature were admitted electively to the PICU for bronchoscopy, whereas our service was aimed at patients with a primary PICU diagnosis; (c) the indications for bronchoscopy among non-elective patients were not always clear; and (d) complications were often expressed as grouped data (e.g. average change in respiratory variables), which may conceal significant instability in individual patients.
With this in mind, we devised a clinically based guideline to aid in identifying PICU patients for whom a bronchoscopy may be indicated. In this report we document the diagnostic and therapeutic yield as well as the complication rate of flexible bronchoscopy using this approach over a 2.5-year period following the commencement of an intensivist-led service in the PICU.
Patients and methods
Between January 2002 and June 2004, 148 bronchoscopic procedures (134 patients) were retrospectively identified from a total of 2564 patient episodes (2427 patients) to the PICU (5.4%). The breakdown of patients undergoing bronchoscopy as a proportion of overall case mix in the PICU was: general paediatrics (77 of 795, 9.7%), cardiac surgery (18 of 754, 2.4%), cardiology (13 of 456, 2.9%), paediatric and orthopaedic surgery (0 of 166, 0%), ENT (17 of 139, 12.2%), nephrology (1 of 54 1.9%), oncology (8 of 39, 20.5%) and other (0 of 24, 0%). Eighty percent of admissions required mechanical ventilation (2052 of 2564) with a reintubation rate of 8.9% (183 of 2052). All bronchoscopies were performed in the acute PICU setting; patients admitted solely for the purpose of an elective flexible bronchoscopy or an intra-operative bronchoscopy were excluded from analysis (n = 9). Data were obtained from the PICU database and medical case note review. Risk of mortality was assessed with the Paediatric Index of Mortality score (PIM2) [13]. The study was conducted in accordance with institutional guidelines.
Indications for requesting flexible bronchoscopy were clinically based, and included four categories (defined prior to the bronchoscopy):
-
1.
Upper airway disease. This comprised the region from mouth, oropharynx and larynx to the sub-glottis and proximal trachea. This category encompassed patients with upper airway obstruction in whom viral croup was unlikely to be the primary diagnosis, including those with a very young age (< 6 months) at presentation, history of intubation and ventilation in the neonatal period (particularly if ex-premature), stridor preceding the acute presentation, presence of cutaneous haemangioma or orofacial abnormalities and patients requiring intubation with a known or suspected difficult airway.
-
2.
Lower airway disease. This comprised suspected pathology of the intrathoracic airway from trachea to the major and segmental bronchi. This was often associated with significant hypercarbia. Indications included mucus plugs in asthma, plastic bronchitis (both for diagnosis and treatment using intratracheal DNAse), acute lobar atelectasis causing significant hypoxia, chronic lobar atelectasis and suspicion of vascular airway compression syndromes.
-
3.
Pulmonary disease. This included investigation of diffuse pulmonary infiltrates (primarily via bronchoalveolar lavage), and pulmonary haemorrhage.
-
4.
Extubation failure. Here bronchoscopy was performed in the immediate post-extubation period to identify why separation from the ventilator was unsuccessful. Due to resource limitations, this was not performed for all failed extubations, but primarily for those patients in whom an airway abnormality was suspected, or in whom diagnostic uncertainty existed. For the upper airway this could include multifactorial causes (cerebral palsy, Down's syndrome), suspicion of vocal cord palsy (birth trauma, cardiac surgery) and following ENT surgery. For the lower airway this was based upon elements of the history, examination and prior investigations (development of biphasic stridor, right aortic arch or suggestion of a mediastinal mass on chest X-ray, recent cardiac surgery involving aortic arch or pulmonary artery manipulation).
Procedure, instrumentation and monitoring
Bronchoscopy was performed using a 2.8-mm (Olympus BF-XP260F) or 3.5-mm (Olympus BF-XP40) external diameter bronchoscope which was connected via a digital converter to a video-bronchoscopic unit (Evis 240S system). All patients had venous access, with continuous ECG, blood pressure, oxygen saturation and end-tidal CO2 monitoring. The procedure was performed at the bedside by one of two paediatric intensive care consultants skilled in flexible bronchoscopy. Anaesthesia was provided by an anaesthetist or experienced PICU fellow (for lower risk patients). Spontaneous ventilation was maintained where possible during dynamic airway studies. Anaesthesia was achieved with intravenous propofol (1–2 mg/kg) or inhalation of sevoflurane (0–4%). Fentanyl and pancuronium were used occasionally. Topical lignocaine was not routinely used as it may exaggerate upper airway pathology [14]. The bronchoscope was passed via a laryngeal mask airway (LMA) if the endotracheal tube was < 3.5 mm or if views of the larynx were required [5]. The nasal route was used in spontaneously ventilating patients for upper airway evaluation when possible. Bronchoalveolar lavage was standardised using 1 ml/kg aliquots of saline [15].
A positive bronchoscopic yield was defined as procedure that resulted in diagnosis that explained the clinical condition or that resulted in a change in management. Secondary outcome measures included length of ventilation, length of PICU stay and safety of the procedure. Safety was assessed by the incidence of adverse clinical events including hypoxaemia (reduction in baseline oxygen saturations by 20% or greater), bradycardia (fall from baseline heart rate by 20% or greater) or hypotension requiring fluid boluses of > 10 ml/kg during the bronchoscopic procedure.
Statistical methods
Continuous variables are reported as median (interquartile range) due to non-normality of the data. The Kruskall-Wallis test was used for analysis of continuous data between groups and chi-squared or Fisher's test for categorical variables. A p value of < 0.05 was considered significant. Analyse-it Software (version 1.62) was used for statistical calculations.
Results
Patient characteristics
One hundred forty-eight procedures were performed on 134 patients; the majority (88%) were mechanically ventilated, and 32 of 148 (22%) were receiving inotropic infusions. Patient demographics for the four clinical groups based on indication for bronchoscopy are shown in Fig. 1 and Table 1. The median (IQR) age and weight was 16.5 months (range 4–75 months) and 10 kg (range 4.5–20 kg), respectively. The median (IQR) length of ventilation in PICU was 3.0 days (range 1.3–5.0 days) with 12 patients (eight with vascular airway compression) invasively ventilated for 14 days or more. There were eight deaths (6%) due to acute respiratory distress syndrome (n = 4), septic shock (n = 2), absent pulmonary valve syndrome (n = 1), and Leigh's syndrome (n = 1).

Bar chart of age distribution between the four clinical groups undergoing bronchoscopy (age under 1 year, between 1 and 5 years and above 5 years)
Yield of Bronchoscopic Procedure
Overall a positive bronchoscopic yield was identified in 113 of 148 (76%) procedures, which varied between 44% (pulmonary disease) to 90% (extubation failure; Fig. 2). The yield of flexible bronchoscopy according to clinical indication was as follows:
-
1.
Upper airway group (84% yield). The majority of bronchoscopies (29 of 32) were performed within 24 h of PICU admission to establish a definitive diagnosis. Thirteen cases were associated with acute stridor following an infective prodrome (presumed viral croup), five of which required revision of the diagnosis to epiglottitis (n = 1), bacterial tracheitis (n = 3) and subglottic cyst (n = 1). Dynamic airway studies in patients with cerebral palsy demonstrated multi-level obstruction (oropharyngeal incompetence with laryngomalacia; n = 5). Four of the five normal procedures were to exclude foreign body inhalation.
Fig. 2 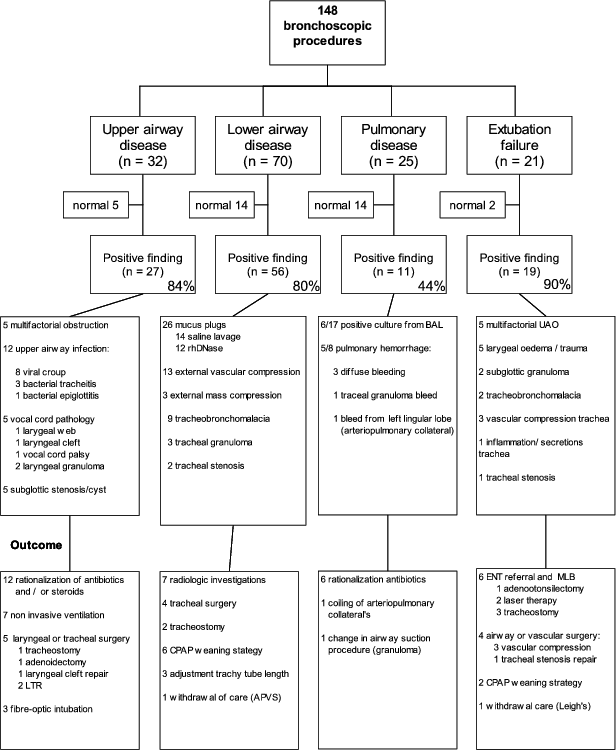
Organisation chart demonstrates the bronchoscopic yield and outcome according to the four clinical groups (upper airway, lower airway, pulmonary disease and extubation failure). UAO upper airway obstruction, LTR laryngotracheal reconstruction, MLB rigid microlaryngobronchoscopy, CPAP continuous positive airway pressure
-
2.
Lower airway group (80% yield). Extensive mucus airway plugging was demonstrated in 26 patients, which was successfully treated with saline lavage (12 of 14) or intratracheal rhDNase administration (12 of 12). In the remaining cases, tracheal or bronchial obstruction was due to extrinsic compression due to vascular structures (n = 13; Table 2), intrathoracic mass lesions (n = 3), tracheo/bronchomalacia (n = 9), stenosis (n = 2) or tracheal granuloma (n = 3).
Table 2 Medical diagnosis, age, weight and site of vascular airway compression. MAPCA major aorto-pulmonary collateral, VSD ventricular septal defect, PA pulmonary artery, LMB left main bronchus, RV right ventricle, RMB right main bronchus -
3.
Pulmonary group (44% yield). A positive microbial agent was identified in only 6 of 17 (35%) BAL's in ventilated patients investigated for diffuse pulmonary infiltrates, all had received antibiotics in the preceding 24 h. The organisms identified were Pseudomonas aeruginosa (n = 4), Enterobacter (n = 1), Aspergillus species (n = 1), Candida (n = 1) and Pneumocystis pneumonia (n = 1). An organism was identified in 42% (3 of 7) of cases in the subgroup of patients with immune suppression (malignancy or HIV). Findings in three of the eight patients investigated for acute pulmonary haemorrhage were non-specific and of no clinical value.
-
4.
Extubation failure group (90% yield). Flexible bronchoscopy was performed in 11.5% of failed extubations (21 of 183). The majority of patients were investigated immediately following the first failed extubation attempt (13 of 21). This was due to upper airway obstruction in ten cases secondary to laryngeal trauma/oedema. Undiagnosed extrinsic vascular compression was identified in three postoperative cardiac surgery patients who failed extubation (Table 2). One patient with a normal bronchoscopy and laryngoscopy had central hypoventilation as a cause for extubation failure, the exclusion of upper airway obstruction facilitating withdrawal of care (Leigh's syndrome). A double aortic arch in a neonate with bronchiolitis who failed extubation was missed on flexible bronchoscopy as the tip of endotracheal tube was below the site of obstruction. This was subsequently identified on rigid bronchoscopy.

Safety
There were no deaths directly related to the procedure. The median Fi02 was 0.4 IQR (range 0.35–0.7 IQR) and oxygen saturations 93% IQR (range 85–97% IQR) prior to bronchoscopy. Transient hypoxia (fall in oxygen saturations by 20%) occurred in 10.8% of cases, the commonest scenario being vascular tracheal compression syndromes (n = 8). Hypoxia occurred in 3 of 18 patients (16.7%) with acute respiratory distress syndrome. One patient with severe tracheal stenosis suffered marked hypoxia and profound bradycardia secondary to rigid chest syndrome following induction with fentanyl. Transient hypotension requiring > 10 ml/kg of 0.9% saline occurred in 26 of 148 procedures (17%); however, this was similar in patients with or without inotropic support (4 of 32 vs 22 of 116; p = 0.6).
Discussion
Traditionally flexible bronchoscopy has been performed by pulmonologists, often on an elective basis in a controlled environment such as PICU or the operating theatre. In this setting, bronchoscopy is a high yield (60–80%), low-risk procedure (complication rate < 1–2%), with < 20% of patients requiring mechanical ventilation [1, 2, 4, 6, 7, 8, 15]. In contrast, our study reports on the application of bronchoscopy from the intensivist's perspective as a tool for diagnosing and treating common respiratory problems in PICU patients. Interestingly, despite the dissimilarity in patient populations, we have shown a comparable yield, at 76% overall. The greater disease acuity among our patients compared with previous studies is evidenced by our proportion of mechanical ventilation (88%) and inotrope administration (22%). Not surprisingly, this was associated with higher complication rates (10% for oxygen desaturation and 17% for hypotension). Nonetheless, the majority of physiological deteriorations were short lived, responded to standard therapy and were not associated with long-term sequelae.
Another difference between our study and previous reports was that we used a clinically based tool to categorise and direct the indications for bronchoscopy. Although this was utilised primarily as a means of rationalising a limited resource, we feel that this approach has also provided valuable data from a clinical perspective, and may be used to inform clinicians of the likely yield when requesting flexible bronchoscopy on similar grounds.
To date, one previous PICU-based study comparable to ours has been published. Bar-Zohar and Sivan report a similar number of bronchoscopic procedures (155 procedures over 2 years), on a broadly similar case mix [11]; however, several important differences between the two studies are apparent. The study reported by Bar-Zohar and Sivan contained a lower proportion of mechanical ventilation (29.6 vs 88%), no cardiothoracic surgical patients were included and a higher proportion of patients had a failed extubation as the reason for bronchoscopy (28 vs 14.2%). Nonetheless, both studies demonstrated a similar yield (76 vs 69%). It is possible that the slightly higher yield in our study was a consequence of case mix, as positive findings as high as 92% have been reported in cardiothoracic surgical patients [16, 17, 18].
In agreement with other authors, we found the greatest yield in patients investigated for upper airway disease (84.3%) and extubation failure (90%) [2, 11]. This is highlighted by the fact that a variety of airway diseases, both acquired and congenital, may present with similar symptoms and signs (e.g. stridor) or even co-exist. Four patients in our study who presented with a clinical diagnosis of bronchiolitis (two were RSV positive) had underlying congenital respiratory tract anomalies (tracheal stenosis, vascular ring, pulmonary artery sling, tracheomalacia). A new diagnosis of vascular airway compression was identified in an additional three patients who had failed extubation.
We also demonstrated a high yield in patients with congenital heart disease. The most severe form of widespread vascular airway compression was seen with absent pulmonary valve syndrome. Common sites of post-operative airway compression were anterior trachea and carina due to enlarged pulmonary arteries or homografts, and left main bronchus compression between aorta and pulmonary artery following hypoplastic aortic arch repair (Table 2). Similar to previous reports, the outcome of these patients is good following surgical intervention to relieve obstruction [16, 17, 18]. Here bronchoscopy is a useful adjunct to radiological imaging, including CT, MRI or bronchography, in delineating the site of obstruction with the advantage of providing dynamic information.
In addition to its diagnostic value we were able to suggest an important therapeutic role for flexible bronchoscopy in removal of central airway plugs with both saline lavage and intra-tracheal rhDNase. Although first described in association with cystic fibrosis, the benefit of intra-tracheal rhDNase in other conditions, such as acute asthma and plastic bronchitis (as seen in sickle cell disease associated acute chest syndrome), is increasingly recognised [19, 20, 21]. The value of flexible bronchoscopy for treatment of atelectasis and mucous plugging is supported by other paediatric studies with a success rate of 40–100% [2, 8, 11, 22, 23]. In a series of 83 children, Holmgren et al. documented mucus plugging as the cause for atelectasis in 65% of cases [22]. In a series of patients with acute sickle chest syndrome, the incidence of plastic bronchitis diagnosed by flexible bronchoscopy was 72% [23]. Accordingly, we advocate a low threshold for flexible bronchoscopy in suspected mucous plugging as the diagnostic yield and therapeutic response is likely to be favourable.
The least useful role for flexible bronchoscopy was for the investigation of pulmonary infiltrates in patients with pneumonitis or ARDS, with identification of an organism occurring in about a third of cases. This low yield is partly explained by the use of broad-spectrum antibiotics, as all patients had been treated for at least 24 h prior to PICU admission. In a number of paediatric studies comprising over 2000 bronchoalveolar lavage samples (including oncology patients), the positive yield varied between 17 and 27% [2, 5, 6, 23, 24], although a higher yield of between 52 and 84% has been reported in selected PICU and oncology patients if done early in the disease process [11, 25, 26]. Similar to reports in adult literature flexible bronchoscopy was not particularly useful for the investigation of pulmonary haemorrhage.
We found flexible bronchoscopy to be safe and with an acceptable complication rate relative to the high disease acuity. There are few studies for direct comparison, as recognised disease acuity scores have not been reported in other studies. Lee et al. [18] found a 36% incidence of transient desaturation in cardiac children investigated with flexible bronchoscopy. In our study, the patients at highest risk for hypoxia were patients with vascular compression syndromes, tracheal stenosis and ARDS; however, we feel that the high yield in this group justified the procedure. In a recent study in critically ill patients, Bar-Zohar and Sivan [11] demonstrated a 20% incidence of hypotension requiring intravascular volume, similar to ours (17%). This compares favourably with a 28.5% incidence of hypotension in acutely ill neonates undergoing bronchoscopy [27]. We found propofol to be a safe agent, particularly in dynamic airway studies, as the anaesthetic and respiratory depression effect is rapidly titratable. The judicious use of fluid boluses prior to the procedure in high-risk cases may have minimised the incidence of hypotension. Similar to others [5], we found that bronchoscopy via a laryngeal mask airway is an effective and safe means of examining the upper airway, particularly in neonates where the endotracheal tubes are too narrow to permit ventilation using the 2.8 mm scope. More importantly, visualisation of the trachea via an endotracheal tube only, may miss upper tracheal pathology (as occurred in our study for a vascular ring in a neonate presenting with bronchiolitis).
This study has several limitations. It is possible that the incidence of physiological deterioration may be underestimated, due to its retrospective nature. The positive yield may be biased upwards by case mix, particularly for cardiac surgery and ENT patients where the likelihood of an airway problem is high. Due to limitations in manpower, only a minority (11.5%) of failed extubations were investigated acutely with flexible bronchoscopy; thus, the true incidence of laryngeal or other airway pathology in this group is unknown. Lastly, and perhaps most importantly for the clinician, we were unable to determine if bronchoscopy had an impact on length of ventilation or intensive care unit stay.
References
Wood RE (2001) The emerging role of flexible bronchoscopy in pediatrics. Clin Chest Med 22:311–317
Nussbaum E (2002) Pediatric fiberoptic bronchoscopy: clinical experience with 2,836 bronchoscopies. Pediatr Crit Care Med 3:171–176
Wood RE, Sherman JM (1980) Pediatric flexible bronchoscopy. Ann Otol Rhinol Laryngol 89:414–416
Perez-Ruiz E, Perez-Frias J, Martinez-Gonzalez B, Martinez-Aran T, Milano-Manso G, Martinez-Valverde A (2001) Pediatric fiberoptic bronchoscopy. Analysis of a decade. An Esp Pediatr 55:421–428
Naguib ML, Streetman DS, Clifton S, Nasr SZ (2005) Use of laryngeal mask airway in flexible bronchoscopy in infants and children. Pediatr Pulmonol 39:56–63
Godfrey S, Avital A, Maayan C, Rotschild M, Springer C (1997) Yield from flexible bronchoscopy in children. Pediatr Pulmonol 23:261–269
de Blic J, Marchac V, Scheinmann P (2002) Complications of flexible bronchoscopy in children: prospective study of 1,328 procedures. Eur Respir J 20:1271–1276
Nussbaum E (1982) Flexible fiberoptic bronchoscopy and laryngoscopy in children under 2 years of age: diagnostic and therapeutic applications of a new pediatric flexible fiberoptic bronchoscope. Crit Care Med 10:770–772
Bush A (2003) Bronchoscopy in paediatric intensive care. Paediatr Respir Rev 4:67–73
Fan LL, Sparks LM, Fix FJ (1988) Flexible fiberoptic endoscopy for airway problems in a pediatric intensive care unit. Chest 93:556–560
Bar-Zohar D, Sivan Y (2004) The yield of flexible fiberoptic bronchoscopy in pediatric intensive care patients. Chest 126:1353–1359
Garcia Garcia E, Perez Ruiz E, Quesada Rodriguez L, Milano Manso G, Perez Frias J, Calvo Macias C, Martinez Valverde A (1999) Usefulness of fiberoptic bronchoscopy in critical paediatric care. Arch Bronconeumol 35:525–528
Slater A, Shann F, Pearson G (2003) PIM2: a revised version of the Paediatric Index of Mortality. Intensive Care Med 29:278–285
Nielson DW, Ku PL, Egger M (2000) Topical lidocaine exaggerates laryngomalacia during flexible bronchoscopy. Am J Respir Crit Care Med 161:147–151
Gibson NA, Coutts JA, Paton JY (1994) Flexible bronchoscopy under 10 kg. Respir Med 88:131–134
Corno A, Giamberti A, Giannico S, Marino B, Rossi E, Marcelletti C, Kirklin JK (1990) Airway obstructions associated with congenital heart disease in infancy. J Thorac Cardiovasc Surg 99:1091–1098
Davis DA, Tucker JA, Russo P (1993) Management of airway obstruction in patients with congenital heart defects. Ann Otol Rhinol Laryngol 102:163–166
Lee SL, Cheung YF, Leung MP, Ng YK, Tsoi NS (2002) Airway obstruction in children with congenital heart disease: assessment by flexible bronchoscopy. Pediatr Pulmonol 34:304–311
Manna SS, Shaw J, Tibby SM, Durward A (2003) Treatment of plastic bronchitis in acute chest syndrome of sickle cell disease with intratracheal rhDNase. Arch Dis Child 88:626–627
Durward A, Forte V, Shemie SD (2000) Resolution of mucus plugging and atelectasis after intratracheal rhDNase therapy in a mechanically ventilated child with refractory status asthmaticus. Crit Care Med 28:560–562
Patel A, Harrison E, Durward A, Murdoch IA (2000) Intratracheal recombinant human deoxyribonuclease in acute life-threatening asthma refractory to conventional treatment. Br J Anaesth 84:505–750
Holmgren NL, Cordova M, Ortuzar P, Sanchez I (2002) Role of flexible bronchoscopy in the re-expansion of persistent atelectasis in children. Arch Bronconeumol 38:367–371
Moser C, Nussbaum E, Cooper DM (2001) Plastic bronchitis and the role of bronchoscopy in the acute chest syndrome of sickle cell disease. Chest 120:608–613
Stokes DC, Shenep JL, Parham D, Bozeman PM, Marienche KW, Mackert PW (1989) Role of flexible bronchoscopy in the diagnosis of pulmonary infiltrates in pediatric patients with cancer. J Pediatr 115:561–567
McCubbin MM, Trigg ME, Hendricker CM, Wagener JS (1992) Bronchoscopy with bronchoalveolar lavage in the evaluation of pulmonary complications of bone marrow transplantation in children. Pediatr Pulmonol 12:43–47
Lanino E, Sacco O, Kotitsa Z, Rabagliati A, Castagnola E, Garaventa A, Dallorso S, Gandolfo A, Manfredini L, Venzano P, Savioli C, Maccio L, Dini G, Rossi GA (1996) Fiberoptic bronchoscopy and bronchoalveolar lavage for the evaluation of pulmonary infiltrates after BMT in children. Bone Marrow Transplant;18:117–120
Schellhase DE, Graham LM, Fix EJ, Sparks LM, Fan LL (1990) Diagnosis of tracheal injury in mechanically ventilated premature infants by flexible bronchoscopy. A pilot study. Chest 98:1219–1225
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Manna, S.S., Durward, A., Moganasundram, S. et al. Retrospective evaluation of a paediatric intensivist-led flexible bronchoscopy service. Intensive Care Med 32, 2026–2033 (2006). https://doi.org/10.1007/s00134-006-0351-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-006-0351-y