
Abstract
Objectives
To compare disease severity as judged by duration of ventilation, inotrope use and mortality in children ventilated for respiratory syncytial virus (RSV)-positive lower respiratory tract infection (LRTI) with and without elevated transaminase levels and to determine the aetiology of elevated transaminase levels in this patient group.
Design
Prospective observational study.
Setting
Twenty-two-bed Paediatric Intensive Care Unit.
Patients
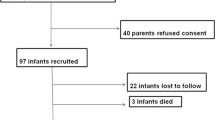
Forty-eight ventilated children with RSV-positive LRTI.
Measurements and results
Alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels were measured daily. In patients with elevated transaminase levels infection with the following viruses was investigated: hepatitis A, B and C viruses, cytomegalovirus, Epstein Barr virus, adenovirus, influenza virus, and parainfluenza viruses (types I, II, and III). Elevated transaminase levels were detected in 22 (46%) patients. The duration of mechanical ventilation (geometric mean; 95% CI) was significantly (P<0.05) longer in the group with elevated transaminase levels: 10.6 (9.4; 11.7) days versus 3.5 (2.8; 4.2) days. This difference remained significant in patients without congenital heart disease. Inotrope use was more common and all deaths occurred in the group with elevated transaminase levels (P<0.05). All patients who died and all but two patients with inotrope requirements had underlying congenital heart disease. One patient with elevated transaminase levels had a simultaneous infection with influenza A virus.
Conclusions
RSV disease in ventilated children was more severe if transaminase levels were elevated. Transaminase level elevation was due to hepatitis in the majority of patients. In patients with congenital heart disease we also detected myocardial involvement.

Similar content being viewed by others


References
Eisenhut M, Thorburn K (2002) Hepatitis associated with severe respiratory syncytial virus positive lower respiratory tract infection. Scand J Infect Dis 34:235
Tristram DA, Miller RW, McMillan JA, Weiner LB (1988) Simultaneous infection with respiratory syncytial virus and other respiratory pathogens. AJDC 142:834–836
Soldin SJ, Hicks JM (eds) (1995) Pediatric reference ranges. AACC, Washington, pp 3,34
Shann F, Pearson G, Slater A, Wilkinson K (1997) Paediatric index of mortality (PIM): a mortality prediction model for children in intensive care. Intensive Care Med 23:201–207
Nadal D, Wunderli W, Meurmann O, Briner J, Hirsig J (1990) Isolation of respiratory syncytial virus from liver tissue and extrahepatic biliary atresia material. Scand J Infect Dis 22:91–93
Fishaut M, Tubergen D, McIntosh K (1980) Cellular response to respiratory viruses with particular reference to children with disorders of cell mediated immunity. J Pediatr 96:179–186
Henrion J, Minette P, Colin L, Schapira M, Delannoy A, Heller FR (1999) Hypoxic hepatitis caused by acute exacerbation of chronic respiratory failure: a case-controlled, hemodynamic study of 17 consecutive cases. Hepatology 29:427–433
Mace S, Borkat G, Liebman J (1985) Hepatic dysfunction and cardiovascular abnormalities. AJDC 139:60–65
Missov E, Mair J (1999) A novel biochemical approach to congestive heart failure: cardiac troponin T. Am Heart J 138:95–99
Huang M, Bigos D, Levine M (1998) Ventricular arrhythmia associated with respiratory syncytial virus infection. Pediatr Cardiol 19:498–500
Thomas JA, Raroque S, Scott WA, Toro-Figueroa LO, Levin DL (1997) Successful treatment of severe dysrhythmias in infants with respiratory syncytial virus infections: two cases and a literature review. Crit Care Med 25:880–886
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Eisenhut, M., Thorburn, K. & Ahmed, T. Transaminase levels in ventilated children with respiratory syncytial virus bronchiolitis. Intensive Care Med 30, 931–934 (2004). https://doi.org/10.1007/s00134-004-2236-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-004-2236-2