
Abstract
Objective
To examine patient-ventilator interaction during pressure support ventilation in critically ill patients when they were ventilated: (1) by a new system (Vision, Respironics) which uses the flow waveform as a method of triggering and cycling; and (2) by a new generation ventilator (Evita 4, Drager) which uses the traditional flow triggering (2 l/min) and cycling criterion (25% of peak flow).
Design
Prospective clinical and bench study.
Methods
Twelve mechanically ventilated patients were studied at three levels of pressure support, applied randomly with both ventilators. The two systems of triggering were further studied at controlled levels of dynamic hyperinflation and respiratory drive using an active lung model.
Results
Patients' breathing patterns, respiratory effort, and arterial blood gases were not affected by the type of ventilator. The flow waveform method of triggering was more sensitive to patient effort than the flow triggering, resulting in less ineffective effort but a greater number of auto-triggerings. At controlled levels of dynamic hyperinflation and inspiratory effort the simulated patient effort needed to trigger the ventilator was considerably less with the flow waveform method of triggering than that with the flow triggering. The flow waveform method of cycling resulted in mechanical breaths with similar characteristics to those that used the traditional flow criterion of breath termination.
Conclusions
We conclude that the flow waveform method of triggering improves the ventilator function and decreases the patient effort during the triggering phase. This system is highly sensitive, but under certain circumstances may be unstable.
Similar content being viewed by others


Introduction
During assisted modes of support the trigger variable and cycling criterion are important determinants of patient-ventilator interaction [1, 2, 3]. It has been shown that both factors may considerably affect the function of the ventilator as well as the patient work of breathing [1, 2, 3, 4, 5]. The trigger variable is usually pressure or flow and the latter is associated with reduced work of breathing during the triggering phase [1, 6, 7]. The cycling criterion depends mainly on the mode of support. With volume assist the cycling criterion is volume or time, whereas with pressure support it is either an absolute value of inspiratory flow or a percentage of peak inspiratory flow [8].
Theoretically, the pressure support mode has the advantage over the assist-volume mode in that the patient retains his/her ability to control the tidal volume and the inspiratory time. Although this might be true in patients with a normal respiratory system, in the presence of abnormal respiratory system mechanics the patient's ability to control these two aspects of breathing is seriously compromised [9, 10]. Furthermore, the work of breathing needed to trigger the ventilator may be substantial, whereas under certain circumstances it may not be adequate to initiate the mechanical breath (ineffective effort) [11, 12]. This has been observed both with pressure and flow triggering systems.
Recently, a new microprocessor-controlled positive pressure ventilatory assist system has been introduced (BiPAP Vision, Respironics) in the market, which incorporates new algorithms to trigger the ventilator and terminate the inspiration during pressure support mode. With these algorithms, designed to improve patient-ventilator interaction, the flow waveform is mainly used to trigger and cycle the ventilator (see below). However, this method of triggering and termination of mechanical breath has not been tested in mechanically ventilated patients. The aim of this study was, therefore, to examine the patient-ventilator interaction during pressure support ventilation in critically ill patients when they were ventilated: 1) by the new system; and 2) by a new generation ventilator (Evita 4, Drager) which uses the traditional variables of triggering and inspiration termination. Because the performance of the ventilator may be affected by confounding factors related to the patient, an active lung model was used and the two systems were studied at controlled levels of dynamic hyperinflation and inspiratory effort.
Methods
Clinical study
Twelve patients admitted to the Intensive Care Unit for management of acute respiratory failure were studied. At the time of the study all patients were hemodynamically stable and ventilated on pressure support (PS) mode through cuffed endotracheal tubes. The PS and positive end-expiratory pressure (PEEP) levels were determined by the primary physician who was not involved in the study (baseline PS). All patients were lightly sedated with propofol (1.0–1.5 mg·kg·h). The level of sedation was such as to achieve a score of 3 in Ramsay's scale [13]. Patients with one of the following characteristics were excluded: 1) pneumothorax with active chest tube leaks; 2) chest wall abnormalities (i.e., kyphoscoliosis); and 3) overt pleural effusion. The study was approved by the Hospital Ethics Committee and informed consent was obtained from the patients or their families.
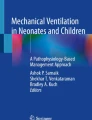
The patients were studied in semi-recumbent position (>45 degrees). In all patients, esophageal pressure (Pes) was measured with an esophageal balloon positioned at the lower third of the esophagus and filled with 0.5 ml of air. The proper position of the balloon was verified using the occlusion test [14]. In random order the patients were ventilated on PS either with the Evita 4 (Drager, Germany) or with the BiPAP Vision ventilators. With both types of ventilators the fractional concentration of O2 (FiO2) and PEEP were similar and equal to those prescribed by the primary physician before the study, whereas the rising time of PS was set to 0.1 s. A single tube and an exhalation valve were used to connect the Vision ventilator to the endotracheal tube, whereas with Evita 4 a commercial ventilator circuit system consisting of a Y-connector and separate ventilator tubes for inspiration and expiration were applied. All tubes had similar length and inner diameter. With both ventilators a heat and moisture exchange filter was used (Hygrobac S, Mallinckrodt, resistance 2.8 cmH2O·l·s, dead space 51 ml). With Evita 4 the threshold for triggering and the cycling criterion were set at 2 l/min and 25% of peak inspiratory flow, respectively. We did not further decrease the threshold for triggering in order to avoid auto-triggering [15]. With Vision the triggering of the ventilator occurred either when patient effort generated inspiratory flow causing 6 ml of volume to accumulate above baseline flow (volume method) or when the patient inspiratory effort distorted the expiratory flow waveform to a certain extent, whichever occurred first. The latter method of triggering is based on the flow waveform and referred to as the shape signal method. This method is based on the generation of a new flow signal (flow shape signal) by offsetting the signal from the actual flow by 0.25 l/s and delaying it for a 300-ms period. The intentional delay causes the flow shape signal to be slightly behind the patient's flow rate. As a result, a sudden decrease in expiratory flow due to inspiratory effort crosses the shape signal and this triggers the ventilator (Fig. 1). The shape signal method is also used to terminate the inspiration. Relaxation of inspiratory muscles and/or contraction of expiratory muscles results in an acute decrease in inspiratory flow which may cross the corresponding inspiratory flow shape signal causing termination of the mechanical inspiration (Fig. 1). In cases where this acute distortion of inspiratory flow does not occur, mechanical inspiration is terminated by an electronic signal that rises in proportion to flow rate on each breath, a method called spontaneous expiratory threshold. When the electronic signal and actual patient flow values are equal, the unit cycles to PEEP (Fig. 1).

Flow-time waveform in two patients ventilated with Vision on pressure support mode. Open arrows: Flow shape signal, generated by offsetting (0.25 l/s) and delaying (300 ms) the actual flow (thick line) during inspiration and expiration. Closed arrows: Electronic signal rising in proportion to actual inspiratory flow (thick line) in each breath. A: Mechanical breath triggered and terminated by the shape method. During expiration the actual flow decreased abruptly (due to the onset of inspiratory effort), crossed the flow shape signal and triggered the ventilator. During inspiration the acute decrease of inspiratory flow caused the actual flow to cross the flow shape signal and terminated the pressure delivery (cycling off) before the electronic signal equalled the actual flow. B: Mechanical breath triggered by the volume method and terminated by the spontaneous expiratory threshold. During expiration the actual flow did not cross the flow shape signal (the actual flow crossed the shape signal after the triggering). The ventilator was triggered when 6 ml of volume was inspired. During expiration the electronic signal equaled the actual flow and terminated the pressure delivery (cycling off) before the actual flow crossed the shape signal flow
With each type of ventilator the patients were studied at three levels of PS (baseline, baseline+5 cmH2O, baseline−5cmH2O) applied randomly. At each pressure level the patient was ventilated for 30 min, whereas arterial blood gases were measured at the end of this period.
At the end of the study the patients were placed on volume-control mode and ventilated with VT between 0.5 and 0.6 l given with a square-wave flow-time profile. In addition, the level of sedation was increased (propofol 6 mg·kg·h plus fentanyl 2.5 μg·kg·h) so as to achieve a score of 6 in Ramsay's scale [13]. Thereafter, a neuromuscular blocking agent was administered (atracurium 25 mg) to inhibit respiratory muscle activity. The absence of respiratory muscle activity was based on specific criteria [16]. When passive ventilation was obtained total respiratory system, and lung and chest wall mechanics were measured by the technique of rapid airway occlusion using standard formulas [17]. All the respiratory mechanics data were computed as an average of three measurements obtained by respective maneuvers satisfying passive condition [16].
Flow (V') at the airway opening was measured with a heated pneumotachograph (Hans-Rudolf 3700, Kan., USA) and a differential pressure transducer (Micro-Switch 140PC, Honeywell, Ontario, Canada), placed between the endotracheal tube and the Y-piece of the Evita ventilator or the Vision exhalation valve. V' was electronically integrated to provide volume (V). Airway pressure (Paw; Micro-Switch 140PC, Honeywell) was measured from a side port between the pneumotachograph and the endotracheal tube. Pes (Micro-Switch 140PC, Honeywell) was measured from the esophageal balloon. Each signal was sampled at 150 Hz (Windaq Instruments, Ohio, USA) and stored on a computer disk for later analysis.
Data analysis
The beginning of inspiratory effort was defined as the time (zero time) of a rapid decrease in Pes. Data over the last 2 min of each 30 min period were used. In each breath V', V, Paw, and Pes were aligned at zero time. Thereafter, pressure generated by all respiratory muscles (Pmus) was calculated from Pes taking into account the passive elastic and resistive properties of the chest wall measured at the end of the study. This calculation, which is based on the Campbell diagram, was described in detail earlier [18, 19, 20].
With this approach Pmus was forced to be zero at zero time. Neural inspiratory time (TIn) was measured as the interval between the beginning of inspiration and the point at which Pmus started to decline rapidly [19, 20]. The intrinsic PEEP (PEEPi) was measured as the portion of Pmus dissipated to reverse flow from expiratory to inspiratory. Mechanical inspiratory (TIm) and expiratory (TEm) time were measured as the interval between the beginning and the end of inspiratory and expiratory flow, respectively. Ineffective efforts and mechanical breaths triggered without inspiratory effort (auto-triggering) were identified from the Pes waveform and expressed as attempts/min and breaths/min, respectively.
We also calculated various indices of respiratory motor output using the Pmus waveform. These indices were:
-
1.
The rate of rise of Pmus (dp/dt); the difference between peak Pmus and Pmus at the onset of neural inspiration (which by definition was zero) divided by the corresponding time.
-
2.
Respiratory muscle effort during the respiratory cycle. This was quantified using the time integral of respiratory muscle pressure [19, 20 , 21]. The time integral of positive and negative Pmus represented the pressure time product (PTP) of inspiratory (PTPi) and expiratory (PTPe) muscles, respectively [21]. PTP of all respiratory muscles (PTPTOT) was calculated as the sum of PTPi and PTPe. PTPi, PTPe, and PTPTOT were calculated on a per breath basis. PTP of ineffective efforts (if present) was also calculated (PTPineffective). PTPTOT per min was calculated as the product of PTPTOT and ventilator frequency. In patients in whom ineffective efforts were observed PTPineffective per min was calculated as the product of PTPineffective and the number of ineffective efforts per min. PTPi was further analyzed by calculating the inspiratory effort dissipated to trigger the ventilator (PTPtrig). PTPtrig was calculated as the time integral of Pmus from the beginning of inspiration to the nadir value of Paw.
The performance of the ventilator was evaluated by: 1) the time delay between the onset of inspiratory effort to nadir Paw (triggering delay); 2) the maximal drop of Paw (ΔPaw) during the process of triggering; 3) the area of Paw-time tracing below PEEP (PTPPaw<PEEP); 4) the area of Paw-time tracing during mechanical inspiration starting from PEEP and ending 0.3 s later (PTPPaw>PEEP(0.3)); and 5) the area of Paw-time tracing above PEEP (PTPPaw>PEEP) during mechanical inspiration. PTPPaw<PEEP was further analyzed by calculating the area below PEEP from initial drop of Paw to nadir Paw (PTP1).
With Vision calculating the flow shape signal during expiration and observing that the patient's flow crossed the flow signal when the actual flow was still expiratory (Fig. 1) identified the breaths triggered by the shape method. Although in several breaths the method of cycling was easily identifiable, as shown in Fig. 1, in others the two criteria of cycling occurred almost at the same time making it difficult to recognize with accuracy which algorithm was used to terminate the breath. For this reason no attempt was made to characterize the method of cycling in each mechanical breath.
Lung model study
In order to compare the flow waveform and flow triggering systems at controlled levels of dynamic hyperinflation and inspiratory effort, a two-chamber test lung (Michigan Instruments, Grand Rapids, Mich., USA) was used. One chamber (driving chamber) was connected to and powered by a ventilator (Puritan-Bennett, USA) whereas the other (experimental chamber) was connected to the ventilator being tested (Evita 4 or Vision). Similar to the clinical study, commercial ventilator tubes were used for all connections. V', V, and Paw were measured as described in the clinical study section. The two chambers were connected by a small lifting bar, such that an increase in the pressure inside the driving chamber applied an external force to the experimental chamber, thus creating a decrease in intra-chamber pressure and simulating an inspiratory effort [6]. The elastance (E) and resistance (R) of the experimental chamber were set at 20 cmH2O/l and 10 cmH2O·l·s, respectively. E of the driving chamber was set at a lower value than that of the experimental chamber, causing—after the triggering of the test ventilator—the experimental chamber to be inflated with a rate that was higher than that of the driving chamber. This represents a condition where the patient relaxes his/her muscles immediately upon triggering. PEEP of 8 cmH2O was applied to the experimental chamber, whereas the tested ventilator was set to PS mode with 10 cmH2O above PEEP pressure. These settings were similar to mean baseline settings used in the clinical study. The PS rising time was set to 0.1 s. The driving ventilator was adjusted to deliver a constant inspiratory flow of 40 l/min or 80 l/min, simulating, respectively, a low and high patient respiratory drive. The frequency of the driving ventilator was adjusted such that the experimental chamber did not reach the equilibrium volume at the end of expiration, creating dynamic hyperinflation. On each level of respiratory drive, two levels of dynamic hyperinflation were studied, reflected by the end-expiratory flow (V'end) which was 0.35 l/s and 0.25 l/s, representing, respectively, high and low dynamic hyperinflation. These levels of end-expiratory flow ensured that with Vision all mechanical breaths were triggered by the shape method (Fig. 1). Thus, each ventilator (Evita 4 and Vision) was examined at four experimental conditions: 1) high drive, high end-expiratory flow; 2) high drive, low end-expiratory flow; 3) low drive, high end-expiratory flow; 4) low drive, low end-expiratory flow. The triggering function of Evita 4 was studied with two triggering flow sensitivities, 1 l/s and 2 l/s.
The simulating effort during the triggering phase was quantitated by calculating the pressure applied on the experimental chamber by the function of the driving chamber (Pmussim). At time t from the beginning of experimental chamber inflation, the total pressure applied (Pmussim+Paw) on the experimental chamber was dissipated to overcome the R and E according to equation of motion as follows:
and
where V'(t) and V(t) were flow and volume above end-expiratory chamber volume, respectively, Paw(t) was airway pressure and PEEPi was chamber pressure at the end of expiration. Because expiration was passive, PEEPi was the driving pressure for expiratory flow at the end of expiration and calculated as follows:
In the above calculations all pressures were referred to PEEP. Similar to the clinical study, in each condition the pressure-time product of Pmussim during the triggering phase (PTPtrigsim) was calculated, whereas the triggering performance of the ventilator was assessed by: 1) the triggering delay; 2) ΔPaw; 3) PTPPaw<PEEP; and 4) PTP1.
Statistical analysis
Data were analyzed by multi-factorial analysis of variance for repeated measurements (ANOVA), followed by Tukey's test, if the F value was significant, and non-parametric Mann Whitney U-test where appropriate. A P<0.05 was considered statistically significant. All values are expressed as mean±SE. In the lung model study the mean±SE for the variables were determined from a total of ten consecutive respiratory cycles.
Results
A. Clinical study
Patients' characteristics and baseline ventilator settings are shown in Table 1. For a given level of PS ventilator timing, VT and arterial blood gasses did not differ between ventilators. Independent of ventilator, TIm increased and ventilator frequency decreased significantly with high PS. At low PS, minute ventilation was slightly but significantly higher with Vision than that with Evita. At baseline and high PS, triggering delay was significantly shorter with Vision than that with Evita (Table 2). Independent of PS, ΔPaw, PTPPaw<PEEP, and PTP1 were significantly lower with Vision (Table 2). For a given PS, PTPPaw>PEEP(0.3) and PTPPaw>PEEP did not differ between ventilators.
For a given PS, neural breath timing did not differ between ventilators (Table 3). With Vision, inspiratory and total respiratory effort tended to be higher and PTPtrig lower; the difference, however, was not significant. Independent of ventilator TIn and patients' breathing frequency decreased significantly with high PS. Respiratory drive and patients' respiratory effort decreased significantly with increasing PS. PEEPi did not differ significantly between ventilators as well as a function of PS.
With Vision, in four patients (nos. 2, 3, 4, and 9) all mechanical breaths were triggered by the volume method. The remaining eight patients triggered the ventilator by the shape method in some breaths during at least one level of PS. In this group 68.8±16.2%, 75.0±13.1%, and 23.8±13.4% of the mechanical breaths were triggered by the shape method, respectively with low, baseline, and high PS. The group that triggered the ventilator only with the volume method had significantly lower time-constant of respiratory system (0.54±0.04 s vs 1.00±0.16 s, P<0.05, Mann Whitney U-test). Neither the performance of the ventilator nor PTPtrig differed significantly between breaths triggered with the shape and volume method. Figure 2 shows, in one representative patient, a mechanical breath and calculated Pmus obtained with the Vision (triggered and terminated by the shape method) and Evita ventilators during baseline PS.

Flow, respiratory muscle pressure (Pmus) and airway pressure (Paw) as a function of time in one representative patient during pressure support delivered with Vision (A) and Evita 4 (B). With Vision this mechanical breath was triggered and terminated by the shape signal method. The beginning of neural inspiration was defined as zero time. Triggering of the ventilator (arrows) occurred 120 and 200 ms after the beginning of neural inspiration, respectively, with Vision and Evita 4. Observe also that the drop of Paw during the triggering phase was considerably less with Vision that that with Evita. The better performance of the shape method of triggering occurred despite the fact that with Vision expiratory flow at 0 time was higher (0.33 vs. 0.24 l/s), whereas inspiratory effort was comparable between ventilators. Dotted line: flow shape signal. Long dashed line: electronic signal rising in proportion to actual inspiratory flow
Six patients had ineffective efforts during at least one level of PS (nos. 1, 5, 6, 7, 10, and 12). In this group the number of ineffective efforts was significantly lower (ANOVA) with Vision than that with Evita (Fig. 3A). The PTPineffective/min calculated at high PS (in which the majority of ineffective efforts was observed) averaged 12.5±5.8 cmH2O·s·min with Evita and 8.2±7.1 cmH2O·s·min with Vision (n=6, P>0.05, Mann Whitney U-test). With Vision, four patients exhibited auto-triggering (nos. 3, 4, 7, and 9). Although in these patients the time constant of respiratory system was lower than the group that did not exhibit auto-triggering, the difference was not significant (0.62±0.07 vs 0.96±0.17 s, P>0.05, Mann Whitney U-test). From these four patients, only one (no. 9) had such breaths with Evita. None of the remaining patients had auto-triggered breaths with Evita. The number of breaths with auto-triggering was significantly lower (ANOVA) with Evita (Fig. 3B).

Ineffective efforts and auto-triggering with Evita 4 (x axis) and with Vision (y axis) in patients in whom the above phenomena were observed during at least one level of PS. Low, baseline and high PS are represented by closed circles, open circles and closed triangles, respectively. Ineffective efforts and auto-triggering were mainly observed with high PS. The patient that exhibited the higher number of ineffective efforts (patient no. 10, severe COPD) had also the longer time constant and a significant increase in tidal volume with high PS. In this patient ventilator frequency at high PS was 11.2 breaths/min with Evita and 10.9 breaths/min with Vision. The higher number of auto-triggering was observed in patient no. 7 who decreased considerably his breathing frequency to less than 5 breaths/min at high PS
Lung model study
Variables obtained with flow triggering of 2 l/min did not differ significantly from those of 1 l/min. Thus, for clarity of presentation, only the comparison between the flow triggering of 1 l/min (the most sensitive) and the shape method was shown. In all experimental conditions, Pmussim as a function of time is shown in Fig. 4. For a given inspiratory flow of the driving ventilator Pmussim waveform did not differ significantly between the two ventilators. Therefore, both ventilators were triggered by a similar simulating respiratory effort. The simulated respiratory drive was approximately twofold to tenfold higher that that observed in patients, placing the tested ventilator in more demanding conditions than in the clinical study.

Lung model study: Simulated respiratory muscle pressure (Pmussim) during the triggering phase of Vision and Evita 4 ventilators. Solid lines: Evita 4. Dashed lines: Vision
For a given experimental condition triggering delay, PTPPaw<PEEP, ΔPaw, PTP1, and PTPtrigsim were significantly lower with the shape method of triggering than those with the flow triggering (Table 4).
Discussion
The most important findings of this study can be summarized as follows: 1) the flow waveform method of ventilator triggering (shape or volume method) was more sensitive to patient effort than the flow triggering, resulting in less ineffective efforts but a greater number of auto-triggerings; 2) termination of pressure support using the waveform method (shape or spontaneous expiratory threshold method) resulted in mechanical breaths with similar characteristics to those which used the traditional 25% of peak flow cycling criterion; and 3) the flow waveform method of triggering (shape method) reduced drop airway pressure and trigger delay during simulated demand compared to flow triggering.
In our study we measured Pes and calculated the pressure developed by all respiratory muscles (Pmus) using the Campbell diagram. We believe that the uncertainties associated with our approach are more acceptable than the uncertainties associated with recording respiratory muscle activity using electromyography for reasons that have been reviewed previously [18, 19, 20, 22]. Furthermore, we did not measure transdiaphragmatic pressure because the purpose of the study was to examine the response of the ventilator to changing total respiratory muscle activity. Under this circumstance, Pmus waveform is a better reflection of respiratory muscle activity than transdiaphragmatic pressure [18].
In the Pmus calculation, we assumed that all of the decrease in Pes before inspiratory flow onset was attributed to the inspiratory muscle activity needed to overcome the threshold load imposed by dynamic hyperinflation [21, 23]. This assumption, however, may not be valid in patients with expiratory muscle activity in whom the decrease in Pes might be due, to some extent, to relaxation of expiratory muscle [24]. Thus, PEEPi reflected inspiratory muscle activity or expirator muscle relaxation. We believe that this uncertainty in Pmus calculation should not affect the results of this study. Relaxation of expiratory muscles decreases the alveolar pressure, thus contributing to the triggering process. In some cases where contraction of expiratory muscles decreases the lung volume below the functional residual capacity (determined by PEEP), relaxation of expiratory muscles may, by decreasing the alveolar pressure below PEEP, trigger the ventilator without the contribution of inspiratory muscles. One of the main purposes of the study was to examine the triggering performance of the ventilator during acute decreases in alveolar pressure brought about either by the contraction of inspiratory or by relaxation of expiratory muscles.
Our study showed that for a given PS arterial blood gasses did not differ between ventilators. However, at low levels of PS, minute ventilation was significantly higher with Vision than that observed with Evita, indicating that the efficiency of CO2 removal differed between ventilators. This can be explained by the different systems used to connect each ventilator to the patient. The Vision ventilator uses a single line to connect the patient, whereas the exhaled CO2 is removed through an exhalation valve. It has been shown that such a system is vulnerable to CO2 re-breathing, particularly at low tidal volume [25]. Thus, we believe that with Vision, due to the operation characteristics of the exhalation valve, the functional dead space—particularly at low PS—most likely increased.
Our study clearly demonstrated that patient-ventilator interaction differed considerably between the two triggering systems tested. The number of ineffective efforts was significantly lower when the patients were ventilated with the new system. The occurrence of ineffective efforts depends on the magnitude of dynamic hyperinflation, the strength of patient's inspiratory effort, and the sensitivity of the triggering system [23]. For a given PS in patients in whom ineffective efforts were observed, the tidal volume—a major determinant of dynamic hyperinflation [23]—did not differ between Vision and Evita ventilators. Furthermore, mechanical expiratory time, end-expiratory flow, PEEPi, and expiratory muscles effort were similar. It follows that the magnitude of dynamic hyperinflation most likely was also similar. Finally, respiratory drive as indicated by dp/dt did not differ between ventilators, suggesting a comparable strength of the patient's effort. Although the level of sedation could exaggerate the phenomenon of ineffective efforts, the similar respiratory drive between ventilators excludes the unlikely possibility that alteration in the level of sedation could be the underlining mechanism of the observed difference. Thus, it is reasonable to conclude that the method of the triggering system was the main factor that underlined the difference in the number of ineffective efforts observed between ventilators. Indeed, the triggering system of the Vision ventilator was more sensitive to patient effort than that of Evita; the triggering delay was shorter whereas the Paw decrease and the area below PEEP were lower than those observed with flow triggering.
Although the performance during the triggering phase was better with the Vision triggering system, this was not associated with reduced patient's effort dissipated to trigger the ventilator. However, the inspiratory effort during the triggering phase depends not only on the triggering function of the ventilator but also on the end-expiratory flow and respiratory drive [2, 3]. These confounding factors may obscure any significant effect of the triggering system on the patient's effort. The situation is further complicated by the different systems used by the two ventilators to remove CO2, which, as already stated, may influence the respiratory drive [5, 19]. Indeed, we observed that, compared to Evita, with Vision the total inspiratory effort and inspiratory effort needed to trigger the ventilator (PTPtrig) changed to the opposite direction. For this reason we carried out the active lung model study and examined the effect of the shape method of triggering both on the performance of the ventilator and on patient's simulated effort during the triggering phase at controlled levels of dynamic hyperinflation (controlled end-expiratory flow) and respiratory drive. The results of the lung model study clearly showed that, compared to flow triggering, at controlled levels of dynamic hyperinflation and respiratory drive, the shape method of triggering was associated with approximately 50% less inspiratory effort needed to trigger the ventilator. This was due exclusively to the triggering delay, which was shorter with the shape method, the difference ranging between 14 ms and 29 ms in various conditions studied. The shorter triggering delay caused an approximately 50% decrease in the airway pressure drop and the area of airway pressure below PEEP (an index of negative work).
It has been shown that during PS the performance of Evita 4 is comparable to all the new generation ventilators tested [26, 27]. Thus, although the flow waveform method of triggering was compared to flow triggering system of Evita 4 ventilator, the results of the current study should also apply to other ventilators, which use the flow triggering method.
The shape method of triggering may not be activated in patients with severe airway obstruction and dynamic hyperinflation. In these patients, due to high expiratory resistance which is usually associated with flow limitation, expiratory flow after an initial peak [28] may drop to relatively low values (less than 0.25 l/s); in which case the flow shape signal has a positive value throughout the remaining expiration and thus the crossing point occurs when the actual flow has an inspiratory direction. This results in inspired volume and thus the volume criterion of triggering which is very sensitive (6 ml) occurs first. Indeed, we have observed several such breaths. It should be possible, however, to activate the shape method of triggering in these patients by decreasing the amount of flow offset. It follows that a system with variable flow offset might solve this problem.
The greater sensitivity of the Vision triggering system resulted in a significantly greater number of auto-triggered breaths. Auto-triggering is a well-known phenomenon inherent to all currently used triggering methods [15, 29]. It has been shown that auto-triggering is associated with low inspiratory drive and breathing frequency, and relatively high stroke volume [15]. In our study, all breaths with auto-triggering were observed with relatively low breathing frequency and absence of dynamic hyperinflation as indicated by the occurrence of zero flow for some time before the beginning of inspiratory effort. The maintenance of zero flow at the end of expiration made the system vulnerable to auto-triggering because of cardiac oscillation, which distorts the airway pressure. With Vision, all auto-triggered breaths occurred only with the volume method of triggering (6 ml of inspired volume). The shape method of triggering requires a relatively large decrease in expiratory flow, which cannot be produced by Paw changes due to random noise or cardiac oscillations. On the other hand, with the volume method, the amount of volume needed to trigger the ventilator is such that may be generated relatively easily by small amplitudes of airway pressure as a result of cardiac oscillations or random noise. With Evita, setting the triggering sensitivity to 2 l/min (or even to 1 l/min) necessitates a much larger amplitude of airway pressure to trigger the breath. Auto-triggering counterbalances the advantages of pressure support ventilation in terms of patient ventilator interaction and may lead to respiratory alkalosis, an important cause of weaning failure and various arrhythmias [9]. Nevertheless, with Vision, the problem of auto-triggering should be easily corrected by simply increasing the volume threshold or by incorporating a flow triggering (with variable flow) in the system. It seems that the triggering system of Vision as it stands may not be suitable to ventilate patients (invasively or non-invasively) with low breathing frequency and respiratory drive and without dynamic hyperinflation.
Expiratory asynchrony is commonly observed during pressure support ventilation [21, 30]. Flow cycling, the primary method for ventilators to terminate the pressure support, may cause either premature or delayed termination of flow, depending on several factors such as the PS level, the flow cycling criterion, respiratory system mechanics, and characteristics of muscle pressure [21, 30]. To minimize the expiratory asynchrony, the new system uses the shape or spontaneous expiratory threshold method to terminate the flow delivery. However, this system of cycling does not seem to offer any significant advantage over the traditional one of flow cycling. For a given PS the mechanical inspiratory time and the area above PEEP during inspiration did not differ between ventilators. Furthermore neural inspiratory time and expiratory muscle effort were also similar between the two systems indicating that the magnitude of expiratory asynchrony was comparable.
The modest decrease in patient effort needed to trigger the ventilator observed with the flow waveform method of triggering is unlikely to be of clinical significance. On the other hand the flow waveform method of triggering by decreasing the likelihood of ineffective efforts may promote patient-ventilatory synchrony with beneficial consequences in the overall patient management [9]. In addition, considering that ineffective efforts during mechanical expiration may be viewed as pliometric contraction (inspiratory muscles contract whereas at the same time lengthen due to continuing decrease in lung volume) the new mode of triggering may be advantageous for inspiratory muscles function. Indeed, recent data have shown that pliometric contraction induces ultrastructural damage to muscle fibers that causes a force deficit [31, 32]. It follows that the process of ineffective triggering during mechanical expiration may cause injury to inspiratory muscles and be a potentially cause of inspiratory muscle weakness and weaning failure. Nevertheless, there is no study in mechanically ventilated patients addressing this important but largely ignored issue.
In conclusion our study showed that compared to traditional method of flow triggering the flow waveform method of triggering improved the ventilator performance, decreased the patient effort needed to trigger the ventilator and reduced the number of ineffective efforts. However, this system as it stands is highly unstable under certain circumstances and this may have serious consequences for patient-ventilator interaction.
References
Giuliani R, Mascia L, Recchia F, Caracciolo A, Fiore T, Ranieri VM (1995) Patient-ventilator interaction during synchronized intermittent mandatory ventilation. Effects of flow triggering. Am J Respir Crit Care Med 151:1–9.
Sassoon CS, Gruer SE (1995) Characteristics of the ventilator pressure- and flow-trigger variables. Intensive Care Med 21:159–168.
Sassoon CS, Foster GT (2001) Patient-ventilator asynchrony. Curr Opin Crit Care 7:28–33.
Branson RD, Campbell RS, Davis K, Jr., Johnson DJ, 2nd (1994) Comparison of pressure and flow triggering systems during continuous positive airway pressure. Chest 106:540–544.
Mitrouska J, Xirouchaki N, Patakas D, Siafakas N, Georgopoulos D (1999) Effects of chemical feedback on respiratory motor and ventilatory output during different modes of assisted mechanical ventilation. Eur Respir J 13:873–882.
Aslanian P, El Atrous S, Isabey D, Valente E, Corsi D, Harf A, Lemaire F, Brochard L (1998) Effects of flow triggering on breathing effort during partial ventilatory support. Am J Respir Crit Care Med 157:135–143.
Nava S, Ambrosino N, Bruschi C, Confalonieri M, Rampulla C (1997) Physiological effects of flow and pressure triggering during non- invasive mechanical ventilation in patients with chronic obstructive pulmonary disease. Thorax 52:249–254.
Chatburn RL (1992) Classification of mechanical ventilators. Respir Care 37:1009–1025.
Georgopoulos D, Roussos C (1996) Control of breathing in mechanically ventilated patients. Eur Respir J 9:2151–2160.
Younes M (1993) Patient-ventilator interaction with pressure-assisted modalities of ventilatory support. Sem Respir Med:299–322
Giannouli E, Webster K, Roberts D, Younes M (1999) Response of ventilator-dependent patients to different levels of pressure support and proportional assist. Am J Respir Crit Care Med 159:1716–1725.
Nava S, Bruschi C, Rubini F, Palo A, Iotti G, Braschi A (1995) Respiratory response and inspiratory effort during pressure support ventilation in COPD patients. Intensive Care Med 21:871–879.
Ramsay MA, Savege TM, Simpson BR, Goodwin R (1974) Controlled sedation with alphaxalone-alphadolone. Br Med J 2:656–659.
Baydur A, Behrakis PK, Zin WA, Jaeger M, Milic-Emili J (1982) A simple method for assessing the validity of the esophageal balloon technique. Am Rev Respir Dis 126:788–791.
Imanaka H, Nishimura M, Takeuchi M, Kimball WR, Yahagi N, Kumon K (2000) Autotriggering caused by cardiogenic oscillation during flow-triggered mechanical ventilation. Crit Care Med 28:402–407.
Prechter GC, Nelson SB, Hubmayr RD (1990) The ventilatory recruitment threshold for carbon dioxide. Am Rev Respir Dis 141:758–764.
D'Angelo E, Robatto FM, Calderini E, Tavola M, Bono D, Torri G, Milic-Emili J (1991) Pulmonary and chest wall mechanics in anesthetized paralyzed humans. J Appl Physiol 70:2602–2610.
Georgopoulos D, Mitrouska I, Webster K, Bshouty Z, Younes M (1997) Effects of inspiratory muscle unloading on the response of respiratory motor output to CO2. Am J Respir Crit Care Med 155:2000–2009.
Xirouhaki N, Kondili E, Mitrouska I, Siafakas N, Georgopoulos D (1999) Response of respiratory motor output to varying pressure in mechanically ventilated patients. Eur Respir J 14:508–516.
Kondili E, Prinianakis G, Anastasaki M, Georgopoulos D (2001) Acute effects of ventilator settings on respiratory motor output in patients with acute lung injury. Intensive Care Med 27:1147–1157.
Jubran A, Van de Graaff WB, Tobin MJ (1995) Variability of patient-ventilator interaction with pressure support ventilation in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 152:129–136.
Fernandez R, Mendez M, Younes M (1999) Effect of ventilator flow rate on respiratory timing in normal humans. Am J Respir Crit Care Med 159:710–719.
Leung P, Jubran A, Tobin MJ (1997) Comparison of assisted ventilator modes on triggering, patient effort, and dyspnea. Am J Respir Crit Care Med 155:1940–1948.
Lessard MR, Lofaso F, Brochard L (1995) Expiratory muscle activity increases intrinsic positive end-expiratory pressure independently of dynamic hyperinflation in mechanically ventilated patients. Am J Respir Crit Care Med 151:562–569.
Lofaso F, Brochard L, Hang T, Lorino H, Harf A, Isabey D (1996) Home versus intensive care pressure support devices. Experimental and clinical comparison. Am J Respir Crit Care Med 153:1591–1599.
Richard JC CA, Breton L, Langlais N, Jaber S, Mggiore S, Fougere S, Harf A, Brochard L (2002) Bench testing of pressure support ventilation with three different generations of ventilators. Intensive Care Med:1049–1057
Calzia E, Lindner KH, Stahl W, Martin A, Radermacher P, Georgieff M (1998) Work of breathing, inspiratory flow response, and expiratory resistance during continuous positive airway pressure with the ventilators EVITA- 2, EVITA-4 and SV 300. Intensive Care Med 24:931–938.
Lourens MS, Berg BV, Hoogsteden HC, Bogaard JM (2001) Detection of flow limitation in mechanically ventilated patients. Intensive Care Med 27:1312–1320.
Hill LL, Pearl RG (2000) Flow triggering, pressure triggering, and autotriggering during mechanical ventilation. Crit Care Med 28:579–581.
Yamada Y, Du HL (2000) Analysis of the mechanisms of expiratory asynchrony in pressure support ventilation: a mathematical approach. J Appl Physiol 88:2143–2150.
Devor ST, Faulkner JA (1999) Regeneration of new fibers in muscles of old rats reduces contraction- induced injury. J Appl Physiol 87:750–756.
Hunter KD, Faulkner JA (1997) Pliometric contraction-induced injury of mouse skeletal muscle: effect of initial length. J Appl Physiol 82:278–283.
Author information
Authors and Affiliations
Corresponding author
Additional information
An editorial regarding this article can be found in the same issue (http://dx.doi.org/10.1007/s00134-003-1765-4)
Rights and permissions
About this article
Cite this article
Prinianakis, G., Kondili, E. & Georgopoulos, D. Effects of the flow waveform method of triggering and cycling on patient-ventilator interaction during pressure support. Intensive Care Med 29, 1950–1959 (2003). https://doi.org/10.1007/s00134-003-1703-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-003-1703-5